In this interview segment, Dutch Professor Theo Boer self-identifies as a voluntary euthanasia sceptic.
I interviewed Dutch Professor Theo Boer—Social Professor of Ethics at Theological University, Kampen, the Netherlands, and a Dutch Euthanasia Committee ethicist—about the Netherlands' assisted dying law.
He volunteers that prior to joining a Euthanasia Committee he was an assisted dying sceptic, and remains so.
And yet he warmly endorses the Dutch leglislative model as a good one for other jurisdictions to emulate, a position that he says has become more clear with experience.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
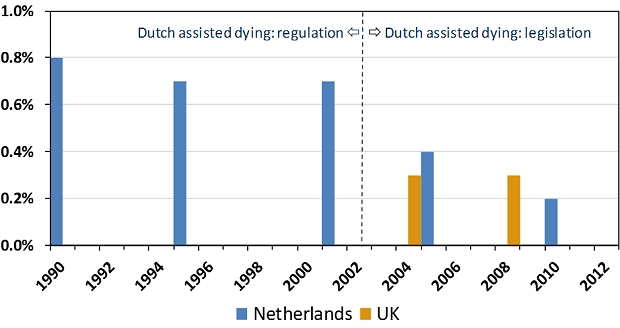
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.
Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
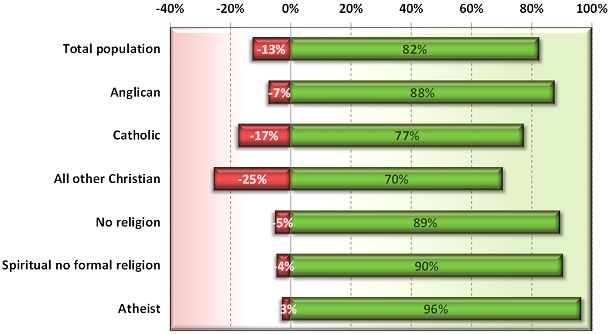
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
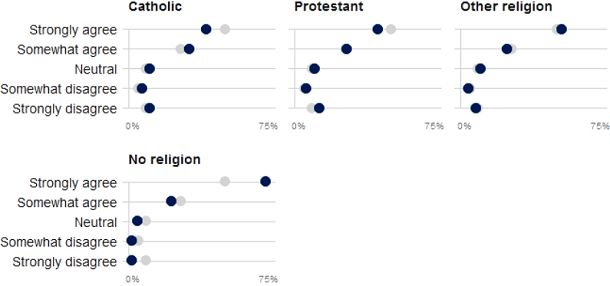
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
Blog by Neil FrancisPosted on Tuesday 8th September 2015 at 5:16am
It was inevitable, the latest attempt by senior British clergy to persuade politicians to reject Lord Joffe’s Assisted Dying for the Terminally Ill Bill. Led by the Archbishop of Canterbury, Justin Welby—whose predecessor Lord Carey now supports the reform—nine clergy sent a letter to ‘remind’ Parliament of supposed terrible consequences.
So what points did the clerics offer to Parliamentarians, and are they valid? Let’s take a look at each of the five ‘reasons’ advanced in order to deny Brits assisted dying choice.
Firstly, the clerics argue that the ‘answer’ is palliative care. Britain boasts the world’s gold standard in palliative care practice and it’s a great credit to practitioners. But the medical literature as well as the experience of the dying and their loved ones is conclusive: palliative care simply can’t always help. Experts say that “relief of suffering remains an elusive goal for many patients” and it’s “clear that improving palliative care will not remove the need for legalizing assisted dying.”
The premise of palliative care is to provide interventions. However, sometimes, not only does interventionism fail to help, it can itself be a source of suffering. And the individual may not want interventions, but rather to alight from the train of terminal illness one or two stops before the inevitable and intolerable terminus.
Secondly, the clerics argue that jurisdictions with assisted dying laws are facing serious problems, including wrongly claiming that the Dutch are now campaigning to include dementia as a basis to seek an assisted death. This right has been enshrined in Dutch law through advance care directives since 2002. In practice, the request is largely declined by doctors.
The clerics complain that dying patients in assisted dying jurisdictions are now using the law—hardly a surprising outcome given the proportion of people now dying of cancer in their later years.
They complain about supposed ‘doctor shopping’ in Oregon. If the patient’s first (or second) doctor declines a request to consider an assisted death on the basis of the doctor’s own convictions, are these clerics suggesting that the patient ought to have their right to lawful assessment denied, because their first doctor or two were religiously opposed?
Thirdly, the clerics argue that the majority of doctors are opposed to assisted dying law reform, ironically pointing out that a quarter to a third of doctors support reform. Why should Brits be denied a choice because two thirds of doctors currently won’t participate in that choice? (What proportion of doctors would participate in abortions, currently legal?) And doctors—who make up fewer than one in two hundred Brits—don’t elect Parliament, so why are their diverse views a case for outright denial?
Let’s name this argument for what it is: an appeal to apparent ‘authority’. Clerical ‘authorities’ (who don’t represent their flocks who are overwhelmingly in favour of reform) are making an appeal of medical ‘authorities’ as the reason to reject something the public believes should be a right. Paternalism indeed.
The fourth argument spreads an icing of hubris on the cake of objections. The clerics argue that the public really don’t understand and don’t know what they mean when the great majority keep saying ‘yes’ to repeated polls on assisted dying law reform.
Public opinion in fact demonstrates the opposite of gullibility: rejection of the attempted scare campaigns of religious ‘authorities’.
Fifthly (and thankfully lastly), the clerics argue that a right to choose assisted dying will inevitably become a duty to choose it. If the theory that ‘a right becomes a duty’ were an argument to reject one right, then all rights would necessarily be rejected on precisely the same principle.
Enshrined in the Mental Capacity Act 2005, Brits already have a right to refuse any medical treatment, even if life-saving. A Jehovah’s Witness may refuse a simple blood transfusion. An elderly person may refuse burdensome surgery. Yet the right to refuse treatment can theoretically become a duty to refuse, in exactly the same manner.
If the clerics genuinely believe their theory then they would argue to Parliament with equal force that the right to refuse medical treatment should be rescinded. Why don’t they?
The real reason for opposing the assisted dying Bill appears in the letter’s preamble: the clerics “hold all human life sacred”, in other words, a ‘gift from God’. Yet contemporary British Social Attitudes surveys reveal that the majority of Brits are not religious.
So the real question for the Parliament is this: should indefensible arguments put forward by a few clerical ‘authorities’ form a basis for denying choice wanted by the overwhelming majority of voters?
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:28pm
The opinion piece in The Age.
In today’s Fairfax press, Sydney woman Mary Ticinovic advances a number of reasons as to why she believes that assisted dying is not merciful. The by-line identifies her as a “clinical psychologist”. But her arguments are not founded on the basic tenets of psychology. How so?
Mary argues that to support assisted dying is to go “against the principle that all life is precious.” She offers no substantive explanation, invoking the notion of ‘human worth’, stating that it exists regardless of the health state or suffering of the person, and complaining that assisted dying promotes the idea that “your life is no longer worth living”.
These are not psychological arguments. We can agree that life is precious. But reluctantly deciding to hasten one’s death in the face of intolerable and unrelievable terminal suffering doesn’t negate that preciousness. Indeed, to some people, choosing assisted dying can evidence the preciousness of one’s very capacities and values as a human.
Whose standards?
Mary further muses over “by whose standards would we judge if life is not worthwhile any more”, as though this is only some vague theoretical argument amongst philosophers or doctors. This is not a psychological argument, either. Under assisted dying law reform, it is only the dying individual’s world-view and circumstances that determine whether he or she feels life is worth living: not anyone else. General philosophical theory doesn’t come into it.
She further argues that assisted dying “promotes a utilitarian view of humanity”. This is not a psychological argument, either. Nor is it valid. Indeed, legalised assisted dying respects the very nature of the diversity of humanity by enabling the world-views many people hold most dear: that of making rational choices consistent with their own beliefs, values and circumstances. Some patients, for example in Oregon, are deeply religious and believe that their God is compassionate and understands and respects their choice to avoid intolerable suffering. That’s not utilitarian at all.
Harm and the Hippocratic Oath
Mary invokes the Hippocratic Oath said by her medical friends to oblige doctors to “do no harm” and that the medical role is “in healing and helping the patient to be restored to health.” This is simplistic nonsense, not a psychological argument.
Firstly, doctors do harm all the time: think of surgical procedures or chemotherapy. Many medical interventions do harm, but we accept the harm because we expect there to be a commensurately greater good as a result.
Secondly, medical practice cannot always “restore the patient to health” as Mary exclusively puts it. What then? The dying patient may judge that the unrelievable suffering they will experience along the path to death is a greater harm than dying a little earlier. And, doctors also have a primary duty to relieve suffering, which Mary doesn’t mention. What is under review is whether a doctor may participate in the relief of intolerable and unrelievable suffering— by hastening death—if the patient believes this is the lesser harm.
Thirdly, the Hippocratic Oath is around 2,300 years old. It requires doctors to swear allegiance to ancient Greek gods. It forbids women from becoming doctors. It requires current doctors to train the next generation free of charge, and it forbids surgery. Contemporary doctors don’t take it, and it’s certainly not “part of training” as Mary mistakenly states.
None of these are psychology arguments.
'Sucker’s choice'
Mary then argues that requiring dying patients to endure until the end promotes—and that assisted dying prevents—“fostering gratitude”, “reconciling hurts or differences with family members or friends” and “showing them strategies or different ways to approach their pain and suffering”.
But, in jurisdictions where assisted dying is legal, for example in Oregon in the USA, these are precisely things that are encouraged under assisted dying. Doctors are required to inform applicants of available medical and palliative interventions. Family gathers on notice of an anticipated death, music and poetry is shared, and expressions of love, devotion and gratitude are exchanged.
If a dying patient has no intention of reconciling with family or reflecting on approaches to dealing with their pain and suffering under an assisted dying law, precisely the same intention applies to the current regime that requires the patient to endure until the end. To assume a difference is a false dichotomy.
Obligatory compassion
Mary also argues that assisted dying ought to remain outlawed because “nursing a sick loved one is a way to give back”. This is yet another specious non-psychology argument. It promotes the ‘right’ of the ‘nurse’ to express love and devotion through ‘caring interventions’ at the expense of the dying patient’s own world view and deeply-held wish for a hastened death. Now who’s being utilitarian?
The upshot
I ran Mary’s opinion piece past an experienced psychologist, who described it as little to do with psychology. Note that neither of us has experience of or is commenting on Mary’s expertise as a clinical psychologist: she may indeed be a very good one.
My associate wondered out loud if Mary’s arguments were based more on underlying religious views than anything else. I agreed: they seemed to me remarkably consistent with the arguments advanced by religious opponents, even though they avoided directly religious words. So I did a little research.
It turns out that Mary is a committed and active Sydney Catholic.* Evidence abounds of her devotion to the Catholic tradition, and I commend her for her conscientious reflective practice and participation in it.
However, I argue that neither the stated psychological qualification nor the unstated religious affiliation make the offered arguments valid.
-----
* By way of fairness, I place on the record that I am agnostic.