Blog by Neil FrancisPosted on Sunday 6th August 2017 at 2:31am
The terminally ill are not choosing between life and death, but between two ways of dying, according to their own beliefs and conscience. Photo: Andrew Drummond/AAP
In Monday’s Herald Sun, Victorian Archbishops Philip Freier and Denis Hart, and Bishops Ezekiel, Suriel, Lester Briebbenow, Bosco Puthur and Peter Stasiuk published a half-page advertisement admonishing the Victorian government for its initiative to legalise assisted dying for the terminally ill, an ad similar to the one published by religious figures in 2008.
I have no quarrel with individuals of faith regarding their own private beliefs. However, the bishops’ attempt at public “leadership” through the advertisement is deserving of redress for its multiple fallacies.
The ‘abandonment’ fallacy
The bishops claimed that assisted dying “represents the abandonment of those who are in greatest need of our care and support”. On the contrary: to ignore the deeply-held beliefs and rigorously-tested wishes of people at the end of life is to abandon their values and critical faculties in favour of the bishops’ own religious dogma.
The ‘competition’ fallacy
The bishops demand there should be more funding for healthcare rather than assisted dying, fallaciously pitting one option against the other. The Victorian government is indeed increasing funding for palliative care. It’s also aiming to provide lawful assisted dying for when even the best palliative care can’t help – which Palliative Care Australia has acknowledged – giving lie to the faux competition.
The evidential fallacy
Contrary to the bishops’ false presumption that legalised assisted dying will decrease trust in “the treatment and quality of care” from doctors, scientific studies into attitude change show that more people trust doctors when assisted dying is legal. Patients can then talk openly about options, even if they decide against assisted death. The bishops have abandoned facts in favour of religious assumptions.
The equivalence fallacy
The bishops refer to assisted dying as “government endorsed suicide”. They fallaciously equate a reasoned, tested and accompanied decision for a peaceful assisted death in the face of a terminal illness, with the impulsive, violent, isolated and regrettable suicide of individuals (many of whom have mental health and substance abuse issues) who are failing to cope with problems that can be addressed.
However, while the latter are choosing between life and death, the terminally ill are choosing not between life and death, but between two different ways of dying, according to their own beliefs and conscience. Rigorous 2016 research from Australian National University shows that the vast majority (79%) of Victorians support assisted dying choice for the terminally ill (with just 8% opposed), clearly distinguishing it from general suicide.
Shame on the bishops for disrespectfully equating the two.
The inconsistency fallacy
They also argue that assisted dying ought to remain prohibited because within healthcare, “mistakes happen and the vulnerable are exploited,” and “that in spite of our best efforts, our justice system could never guarantee” no one would die by mistake or false evidence. However, as I’ve pointed out before, an identical hypothetical problem exists under the refusal of life-saving medical treatment, a statutory right that Victorians have enjoyed for nearly 30 years. The statute has only three “safeguard” requirements, yet even those only apply if the refusal is formally documented, but not if it’s verbal.
Further, the United States Conference of Catholic Bishops directs that patients may refuse treatment if it imposes “excessive expense on the family or community,” yet makes no mention of the hypothetical “vulnerability” of the patient to be persuaded so, nor directs any requirements to assess the veracity of the refusal.
In stark contrast, the Victorian proposal for assisted dying legislation contains more than 60 safeguards and oversights.
The bishops are at risk of ridicule for such a gargantuan flip-flop: supporting the refusal of life-saving treatment with little or no oversight, while vocally opposing assisted dying legislation that mandates an armada of protections.
The not-so-hidden agenda
The bishops’ methods are rather unsubtle – hoping that these arguments, erroneous but carefully crafted to avoid any religious connotations, will be accepted as non-religious. Yet religion is writ large across their plea: as signatories to the letter they are all clerics employed directly and centrally in the promotion of their religions.
The authority fallacy
They might also rely on their religious status to convey gravity and authority to their pleas. Yet as people paid to do a job, like anyone else, their titles grant them no special privileges in lecturing Victorians about how they should die in the face of a terminal illness.
According to the 2016 census, just 23% of Victorians identified as Catholic, 9% as Anglican, 0.5% as Lutheran, and the other bishops’ signatory denominations so small as to not appear separately in the government’s statistics. Combined, the bishops’ faiths represent around 33% of the Victorian population, while 32% of Victorians identify with no faith at all. Surely the bishops are not arguing that they’re speaking for these other Victorians, too?
But the bishops don’t represent the views of their own flocks, either. According to the 2016 ANU study, 89% of non-religious Victorians support assisted dying law reform, as do 78% of Victorian Catholics and Anglicans. Indeed, opposition to assisted dying exists mostly among those who attend religious services once a week or more often – that is, those who are frequently exposed institutional religious messages of opposition – yet who comprise just 12% of Australians and 11% of Victorians.
Minding their own flocks
Australians are abandoning religion in droves. For example, when Freier ascended to the top job of Anglican Primate of Australia in 2006, some 19% of Australians identified as Anglican (2006 census). A decade later under his leadership, the 2016 census showed a drop of about a third to just 13%, and in Victoria, his home territory, to just 9%.
Hart’s Catholic church has experienced a drop in affiliation too, and it’s likely to continue and accelerate as Australians react with shock and disgust to the extent of child sexual abuse that the royal commission has exposed from under his organisation’s “pastoral umbrella”.
In conclusion, rather than bishops lecturing the government and Victorians with fallacious and faintly desperate arguments about the choices they shouldn’t have at the end of life, attending to their own flocks may be more useful Christian leadership.
May their God go with them in that endeavour.
This article was originally published in The Guardian.
To add insult to injury, it flip-flops on its stance.
Never mind that the argument is contradicted by evidence
The Church’s favourite argument — already contradicted by scholarly analysis that curiously seems to be of no interest to the Church — is this: if people are given the choice of assisted dying, they will feel compelled to choose it, coerced by doctors, greedy relatives or others; subtly or otherwise.
No matter that health care workers routinely report that relatives usually try and persuade their dying loved one to endure yet another invasive and burdensome treatment; not dissuade them from it.
The flip-flop
If the Catholic Church were indeed genuinely concerned about coercion of ‘the vulnerable,’ then it would equally oppose the right to refuse medical treatment, particularly if the treatment were life-prolonging. But it doesn’t.
If granny might die as a result of refusing a particular medical intervention, then a doctor might persuade her to refuse in order to conserve medical resources. Or greedy relatives might persuade her so that they are relieved of the burden and expense of looking after her and gain earlier access to her estate.
As eminent legal scholar Gerald Dworkin has argued,1 if there’s a theoretical ‘slippery slope’ for assisted dying, it’s the same for the refusal of life-preserving medical treatment.
To hold different positions under the same risks is to flip-flop. That’s especially so when there are numerous safeguards built into assisted dying statutes, but currently few or none for the right to refuse life-preserving medical treatment.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
Local experience confirms risk is theoretical
In my home state of Victoria, where the right to refuse any unwanted medical treatment has been enshrined in statute for nearly three decades (the Medical Treatment Act 1988), how many prosecutions have there been under the Act’s provisions against inappropriate persuasion?
Precisely none. Not a single case. So much for the theory.
It all serves to highlight that the Catholic Church’s only real argument is that it believes that it’s morally wrong to deliberately hasten death. However, it avoids this argument because as a religious tenet, it doesn’t appeal to the masses.
Catholic directives
The Church’s flip-flop about ‘the vulnerable’ is not a one-off accident. Take for example the ‘Ethical and Religious Directives for Catholic Health Care Services’ published by the United States Conference of Catholic Bishops.2
The Bishops ‘direct’ that there is no obligation on patients to use disproportionate means of preserving life. They state that disproportionate means are:
“…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
The Bishops further ‘direct’ that:
“The free and informed judgment made by a competent adult patient concerning the use or withdrawal of life-sustaining procedures should always be respected and normally complied with, unless it is contrary to Catholic moral teaching.”
Setting aside the Church’s hubris of dishonouring the patient’s choice if the Church disagrees, it would be theoretically easy for someone to persuade the patient that hope was not reasonable, that the burden would be too great, or that the cost to the family or society would be too high.
Suffering for our God’s (your own) good
On the next page, the Bishops expressly ‘direct’ that:
“Patients experiencing suffering that cannot be alleviated should be helped to appreciate the Christian understanding of redemptive suffering.”
That’s unqualified. So, if you’re atheist, agnostic, Jewish, Hindu, Muslim or even a Christian who believes assisted dying can be appropriate, as a patient in their institutions you are to be persuaded that suffering against your beliefs and wishes is ‘redemptive’ in the eyes of the Vatican’s version of a God.
In Australia in 2009, for the Office for Family and Life in the Catholic archdiocese of Adelaide, Mr Paul Russell argued in News Weekly that “there is a point to suffering” because:
“It’s about the profound connection that each and every life has to the incarnate God … We know that the sufferings we endure well are joined in some mysterious way to the sufferings of Christ.”
Pity any poor soul who doesn’t share Mr Russell’s views. Curiously, there is no mention of this underpinning belief in his anti-assisted dying blog, “HOPE.”
Invalid argument in any case
The Church’s argument that ‘the vulnerable’ will be ‘at risk’ from assisted dying laws — for example in the Victorian Bishops’ recent pastoral letter to the Catholics of Victoria opposing the upcoming assisted dying parliamentary Bill — is itself fundamentally invalid.
That’s because, as I’ve previously explained, it’s a circular argument: a logical fallacy.
A circular argument: We must ban yellow socks on Wednesdays or the 'vulnerable' will be 'at risk'.‘The vulnerable,’ by definition are those ‘at risk,’ and will still be so if we wear yellow socks on Wednesdays. Therefore, we should ban such bright footwear midweek — and anything else we happen to oppose — on the same basis.
Might anyone suggest that “we should ban religion because the vulnerable will be at risk of succumbing to extreme religious views”?
Will the Church change its mind?
The Catholic Church does change its mind from time to time, though its reforms are glacially slow.
Take, for example, its theory of limbo, a place on the doorstep of hell where, the Church claimed, babies go if they die before they’re baptised: that they’d be prevented from entering heaven. It would be hard to imagine a crueller worry to put into the heads of uneducated new parents.
But in 2007, after centuries of confidently promoting the theory, the Catholic Church decided that it was wrong and buried it.
Will it change its mind on assisted dying? Maybe, but don’t hold your breath.
Conclusion
The Catholic Church, reeling from its extensive failure to protect our most vulnerable — children — and notwithstanding some good individuals within, still presumes to morally lecture the rest of us with the logical fallacy of how ‘risky’ assisted dying legislation is supposed to be to ‘the vulnerable,’ while flip-flopping in support of refusing life-saving medical treatment under the same theoretical risk.
The Bishops’ rhetoric amply exposes their confected crisis against assisted dying as nothing but religious doctrine draped in faux secular garb… in reality a sheep in wolves’ clothing.
References
Dworkin, G, Frey, RG & Bok, S 1998, Euthanasia and physician-assisted suicide, Cambridge University Press, Cambridge, New York. pp.66ff
Blog by Neil FrancisPosted on Tuesday 20th June 2017 at 9:23pm
Yet more research contradicts Prof. Margaret Somerville's Dutch NVE claim
I’ve criticised Catholic ethicist Professor Margaret Somerville in the past for promoting misinformation about assisted dying. One of her favourite stories is about supposed non-voluntary euthanasia (NVE) ‘contagion’ from voluntary euthanasia laws.
NVE is where a doctor deliberately hastens the death of a patient without a current explicit request from the patient.
Somerville claims that elderly Dutch citizens fear NVE — a slippery slope claim previously promoted by the Vatican. She stated that:
“Old Dutch citizens are seeking admission to nursing homes and hospitals in Germany, which has a strict prohibition against euthanasia because of its Nazi past, and they're too frightened to go into nursing homes or hospitals in the Netherlands.”
She made the claim with certainty and without qualification.
She also stated it under the credentials of Professor, yet has offered not a shred of sound, verifiable evidence. That's unscholarly.
Her claim is premised on two false beliefs, that:
The Dutch assisted dying law causes NVE —extrapolated to mean that elderly Dutch are therefore fearful of NVE in the Netherlands; and
Because assisted dying is illegal in Germany, NVE doesn’t happen there — extrapolated to mean that elderly Dutch are confident in German healthcare and seek it in preference to their own.
Belief 1 is soundly contradicted by the evidence. Researchers have found small but significant rates of NVE in every country they’ve studied (though that to date hasn’t included Germany). They’ve also found that the rates of NVE in the Netherlands and Belgium have dropped (not risen) significantly since their assisted dying laws came into effect in 2002.
Now, new research comprehensively knocks Belief 2 off its perch, too.
In a pilot study just published in the German Medical Weekly, a team led by Professor Karl Beine of Witten/Herdecke University in Germany found that around 3.1% of doctors and nurses surveyed were aware of deliberately hastened deaths (which is illegal in Germany) in the past twelve months, and that 2.4% of them administered it themselves.
A new study has found that of German nurses and doctors who had intentionally administered life-ending drugs to patients (which is against the law), 40% of them had not been asked to do so by the patient: non-voluntary euthanasia. Further, of those who administered it themselves, 40% hadn’t been asked for it by the patient. That's NVE.
While previous evidence strongly suggested that NVE would occur in Germany as everywhere else, this study now factually establishes that it does.
The study authors concluded that “illegal intentional life-ending acts were administered by physicians and nurses in all healthcare areas [hospitals and nursing homes] under investigation.”
So much for Somerville’s second premise.
Now both premises of her misinformed NVE story are soundly contradicted by empirical research evidence.
The F filesPosted on Monday 27th March 2017 at 8:50pm
Dr Michael Gannon announces the AMA's policy review to AMA members in 2015
In 2016, the Australian Medical Association (AMA) reviewed its policy on ‘euthanasia and physician assisted suicide.’ Despite ample evidence to the contrary, the AMA executive set its policy as opposed to assisted dying, when the only position that would have acknowledged and respected the views of most of its membership was a position of neutrality.
The Australian Medical Association (AMA) has been historically opposed to legislative reform that would permit doctor-assisted dying for patients in unremitting and untreatable extremis. Its hostile position had been expressed through a Position Statement (PS) in effect for at least a decade, although its Code of Ethics has been completely silent on the matter.
The AMA’s opposition to doctor-assisted dying has been one of the factors leading to the failure of a number of attempts at assisted dying law reform.
In 2015 the AMA announced a review of its ‘policy’ on ‘euthanasia and doctor assisted suicide,’ managed through its Federal Council. The review was conducted from late 2015 and throughout 2016. It included an online survey of more than 3,700 Australian doctors.
Deeply flawed survey — against assisted dying
The survey methodology contained, however unconsciously, multiple serious design flaws biased against assisted dying: flaws which were brought to the attention of the AMA executive separately by two survey design experts. The executive dismissed the criticisms, incoherently arguing that while the AMA’s reviews are “fully-informed decisions based on well-researched, comprehensive information,” the survey was “not formal ‘research’ as such” and merely a “means to engage our members.”
The AMA relied on selected statistics from the survey to publicly explain the outcome of its review. It also provided its own members a private, detailed report of the review, of which more than half was a comprehensive statistical analysis of the survey.
The ‘Survey Limitations’ section of the report mentioned several minor issues, but not the significant biases brought to the attention of the executive by experts.
Yet supportive doctor responses
Despite these significant biases against assisted dying, the survey found:
68% of doctors said that even with optimal care, complete relief of suffering is not always possible.
60% of doctors said that if lawful, euthanasia should be provided by doctors, and more than half of them (total 32%) said that they would indeed practice it.
52% of doctors said that euthanasia can form a legitimate part of medical care.
50% of doctors expressly disagreed with the AMA’s statement that “doctors should not provide euthanasia under any circumstances.”
38% of doctors expressly disagreed with the AMA’s policy opposed to assisted dying (only half expressly agreed), and 35% of doctors said that euthanasia should be lawful.
Some doctors oppose legalisation, not euthanasia itself
In relation to the last point, other scholarly research has found that an additional 25% of Australian doctors are opposed to law reform not because they are opposed to assisted dying itself, but because they would rather practice it in private without regulatory ‘interference.’ This confirms that more than half of Australian doctors believe assisted dying can be a legitimate and practical part of medical care.
AMA not representative of Australian doctors
Only AMA members were invited and permitted to participate in the survey, and more than 70% of Australian doctors are not AMA members, despite the AMA expressly advancing itself as representing all Australian doctors. Non-members are likely to be more supportive of assisted dying — snubbing AMA membership due to the AMA’s ‘officially’ hostile stance.
Hostile tweets by President during review
During the review process, AMA President Dr Michael Gannon made repeated public statements hostile towards assisted dying, including a statement that doctor assisted dying would offend the Declaration of Geneva. The Declaration has nothing specific to say about assisted dying, and any general Declaration statements Dr Gannon relied upon would be equal arguments against abortion. Yet the AMA accepts abortion practice by doctors.
Indefensible conclusion by AMA Executive
Finally, in the face of ample evidence (despite the methodological biases) that at least half of the AMA’s own members favour doctor involvement in lawful assisted dying and deem it legitimate medical care, and 38% of its own members expressly disagreeing with its opposed policy, the AMA executive decided to maintain ‘official’ organisational opposition in the revised PS.
The PS, which was previously named broadly as about ‘end of life care’, is now exclusively named as about ‘euthanasia and physician assisted suicide,’ even though it continues its broad coverage. This suggests that, however unconsciously, the executive’s attitudes against assisted dying have become more entrenched.
The PS continues to unequivocally state as before that “The AMA believes that doctors should not be involved in interventions that have as their primary intention the ending of a person’s life.” In announcing the conclusions of its review the AMA has promoted this statement widely and as though it applies to all Australian doctors, most of whom are not AMA members.
Neither AMA 'policy' nor its Code of Ethics is binding
Despite the confidence and certainty of the statement, the AMA advises that neither Australian doctors in general nor even its own members are bound by its PSs. Thus, statements in AMA PSs are more ‘suggestions’ or ‘thought bubbles’ rather than authoritative statements.
More recently, the AMA’s Code of Ethics has been updated, yet remains entirely silent on doctor-assisted dying, in curious contradiction of the ‘certainty’ of its PS. The Code of Ethics is not binding on doctors (even AMA members), either.
Incoherent demands for policy consultation
The AMA executive continues to demand deep involvement in the development of a legal framework for assisted dying (despite saying that doctors should not be involved in the practice), yet it has developed no specific frameworks for three other related, already-lawful medical practices: refusal of life-preserving medical treatment, continuous deep sedation until death, and the voluntary refusal of food and fluids.
These discrepancies collectively raise the question as to whether the AMA’s ‘official’ opposition to assisted dying law reform is political rather than medical.
Conclusison
The evidence is clear that the only “justifiable” position the AMA executive could have taken was to declare the AMA neutral towards lawful assisted dying — a matter of individual conscience for its member doctors.
Australian doctors may well question the AMA executive as to how such a flawed process arrived at the outcome it did, and a collection of questions are posed for the AMA to answer. Sixteen questions are posed below.
Why does the AMA, through its Tasmanian representative, think it appropriate to state on national television that dying patients in extremis and without relief can suicide by themselves, even if the AMA doesn’t “encourage” it?
Why did the AMA repeatedly delete corrections to its negative MJA misinformation about assisted dying practice in Belgium?
Why did the AMA decide to review its “policy on euthanasia and physician assisted suicide” when it didn’t specifically have one? It had a policy on the role of doctors in end of life care.
Why did the AMA review comprehensively ignore the substantial secondary data that already exists about the attitudes and practices of doctors and patients in end of life decisions?
Why did the AMA not proactively obtain professional advice and assistance with the design and conduct of its doctor survey, and prefer to use such an amateurish one?
If the AMA really represents all Australian doctors, why did it expressly exclude more than two thirds of them from its survey?
Why did the AMA persistently use inappropriate language and inadequate definitions about assisted dying?
Why did the AMA not make any serious attempt to understand patient perspectives beyond superficial statements that ‘opinions are divided’?
Why did the AMA not report the multiple significant biases in its survey, which it knew about, in the ‘limitations’ section of its final report?
Why did the AMA President consider it appropriate to make multiple statements hostile towards assisted dying while the review was underway?
Why did the AMA executive decide to continue to demand doctors not participate in assisted dying, when more than half of its own members said it could be appropriate clinical practice provided by doctors, nearly four in ten expressly disagreed with the policy, and a third said they’d participate if assisted dying were legalised?
Why does the AMA consider it appropriate to make repeated categorical, public statements that doctors should not be involved in assisted dying, when its Position Statement is not binding on its own members, let alone all Australian doctors?[1]
How can the AMA justify the incoherence of having an expressly opposed stance to assisted dying in its revised Position Statement while it remains totally silent on the matter in its Code of Ethics, revised at the same time?
How can the AMA legitimately demand to be centrally involved in developing an assisted dying framework — in which it says doctors should not be involved — for law reform, when it has no frameworks at all for the similar contexts of refusal of life-preserving medical treatment, continuous deep sedation until death, and the voluntary refusal of food and fluids (all currently lawful and practiced)? When will it develop and publish those?
Why does the AMA continue to present itself to the media and the public as representing all Australian doctors, when more than two thirds of them are not members?
Will the AMA include a formal analysis and critique of this deeply flawed policy review as part of its modernisation efforts in order to rebuild its brand value and stem the falling tide of its membership? That is, is the AMA prepared to learn from its mistakes?
[1] The AMA’s Code of Ethics is not binding even on its own members, either. So when the Code states “don’t engage in sexual, exploitative or other inappropriate relationships with your patients,” that’s merely a ‘suggestion’ or ‘recommendation’ rather than an ‘obligation’ as a member of the AMA.
Blog by Neil FrancisPosted on Sunday 5th March 2017 at 10:24pm
Alex Schadenberg's latest shrill and misleading article
Catholic Canadian anti-assisted-dying blogger Alex Schadenberg is at it again. This time he’s parading his ignorance and spreading bull about a potential change in Oregon’s assisted dying legislation.
The Bill
Mr Schadenberg correctly reproduced Section 3 of Oregon Senate Bill 893, which states:
SECTION 3. An expressly identified agent may collect medications dispensed under ORS 127.815 (1)(L)(B)(ii) and administer the medications to the patient in the manner prescribed by the attending physician if:
(1) The patient lawfully executed an advance directive in the manner provided by ORS127.505 to 127.660;
(2) The patient’s advance directive designates the expressly identified agent as the person who is authorized to perform the actions described in this section;
(3) The patient’s advance directive includes an instruction that, if the patient ceases to be capable after medication has been prescribed pursuant to ORS 127.800 to 127.897, the expressly identified agent is authorized to collect and to administer to the patient the prescribed medication;
(4) The medication was prescribed pursuant to ORS 127.800 to 127.897; and
(5) The patient ceases to be capable.
Mr Schadenberg fails to mention Section 2, which states:
SECTION 2. Section 3 of this 2017 Act is added to and made a part of ORS 127.800 to 127.897.
What is the ORS range?
And what precisely is ‘ORS 127.800 to 127.897’ (ORS = Oregon Revised Statutes)? Why, it’s the entirety of Oregon’s existing Death With Dignity Act!
In other words, a patient still has to be terminally ill, fully informed, made a formal request, the request assessed as genuine and free, waited the required cooling off period, made another formal request, been assessed as qualifying all the requirements by multiple doctors, has legally appointed an agent expressly for the purpose of administering lethal medication pursuant to the Death With Dignity Act, have their medication prescribed (immediately before which the attending physician must again verify that the patient is making an informed decision) and then the patient ceases to be capable, before the agent may then administer.
Mr Schadenberg exposes that at best he fundamentally doesn’t understand the Bill, nor took much if any effort to do so.
That’s hardly the free-for-all Mr Schadenberg posits in his shrill blog implying that ‘assisted suicide and euthanasia’ was being extended to ‘incompetent people’ without further qualification; falsely insinuating that any incompetent person could then obtain assistance for suicide or euthanasia.
No ‘defence’
If Mr Schadenberg were to claim that he really meant ‘only within the scope of the current Death With Dignity Act,’ and that he’s been taken out of context, that simply won’t wash. Bill 893 makes a provision only for someone else to administer the lethal dose (that is, what Mr Schadenberg refers to as ‘euthanasia’) if the patient ceases to be capable after already qualifying under the existing Act. The Bill does not permit patient self-administration: that is, using Mr Schadenberg’s own language, ‘assisted suicide’—which he expressly refers to in his article.
Parading a non-existent extension of ‘assisted suicide’ clearly exposes that at best he fundamentally doesn’t understand the Bill, nor took much if any effort to do so.
Wrong again…
He also got it completely wrong as to who may administer when the patient ceases to be capable:
“The bill enables the doctor to administer…” — Alex Schadenberg
However, if you read Section 3 of the Bill (above) that Mr Schadenberg himself reproduces, you’ll see clearly that the patient must expressly identify a particular person ('agent') to administer lethal medication should the patient cease to be capable. The patient may appoint his or her doctor, but can appoint in their Advance Care Directive anyone to be the agent; including a trusted and loved family member. The only particular requirement for the agent’s administration is that he or she must “administer in the manner prescribed by the attending physician.”
Conclusion
But let’s not the facts get in the way of a gratuitous reaction trumpeting shrill hyperbole and headline, shall we Mr Schadenberg?
And as usual, Catholic Australian anti-assisted-dying blogger Paul Russel has dutifully reproduced Mr Schadenberg’s farce.
Blog by Neil FrancisPosted on Thursday 9th February 2017 at 9:53pm
You only have to look to understand who is campaigning against your right to choose an assisted death in the face of intolerable and unrelievable suffering.
A case in point is a massive advertisement published in both of Melbourne’s daily newspapers: News Corp’s The Herald Sun (right-wing) and Fairfax Media’s The Age (left-wing). The ad was published in 2008 when Victorian MLC Colleen Hartland introduced the Medical Treatment (Physician Assisted Dying) Bill into the State legislature.
The Catholic Archbishop of Melbourne, Denis Hart, also sent the advertisement as a letter to all members of the Victorian Parliament.1
So, who are the advertisement’s signatories? I’ve listed them all in Table 1.
Table 1: Signatories to the 2008 Victorian anti-assisted-dying advertisement
Rt Rev. Graham Bradbeer
Moderator, Presbyterian Church of Victoria
The Rev. Fr Graeme A. Michell, FSSM
Parish Priest, Anglican Catholic Parish of St Mary the Virgin, Melbourne
Rev. Ross Carter
Uniting Church in Australia
Pastor Graham Nelson
Senior Pastor, Life Ministry Centre
Rev. Dr Max Champion
National Chair of the Assembly of Confessing Congregations within the Uniting Church in Australia
Rev. David Palmer
Convenor Church and Nation Committee, Presbyterian Church of Victoria
Pastor Mark Conner
Senior Minister of CityLife Church
Rev. Greg Pietsch
President, Victorian District, Lutheran Church of Australia
Dr Denise Cooper-Clarke
Adjunct Lecturer, Ridley Melbourne Mission and Ministry College
Rabbi Dr Shimon Cowen
Director Institute for Judaism and Civilization
Very Rev. Dr Michael Protopopov
Dean - Russian Orthodox Church in Australia
Rev. Megan Curlis-Gibson
St Hilary’s Anglican Church, Kew
Marcia Riordan
Respect Life Office, Catholic Archdiocese of Melbourne
Archbishop Dr Philip Freier
Anglican Church of Melbourne
Metropolitan Archbishop Paul Saliba
Primate of Antiochian Orthodox Archdiocese of Australia, New Zealand & the Philippines
Imam Riad Galil
West Heidelburg Mosque
Member of the Victorian Board of Imams
Bishop Peter Stasiuk CSSR DD
Eparchy of Saints Peter and Paul of Melbourne, for Ukrainian Catholics in Australia and New Zealand
Rev. Father James Grant SSC
Chaplains Without Borders,
Melbourne Anglican Diocese
Dale Stephenson
Senior Pastor Crossway Baptist Church
Assoc. Professor Afif Hadj MB BS (Melb) FRACS
Director of Surgery, Director of Medical Training, Maroondah Hospital (A Monash University Teaching Hospital)
Pastor Peter Stevens
Victorian State Officer
Festival of Light Australia
Archbishop Denis Hart
Catholic Archdiocese of Melbourne
Dr Nicholas Tonti-Filippini
Associate Dean, JPII Institute for Marriage and Family Melbourne
Rev. Fr Geoff Harvey
Priest of the Good Shepherd Antiochian Orthodox Mission Parish, based at Monash University
Rob Ward
Victorian State Director Australian Christian Lobby
Assoc. Professor Rosalie Hudson
Aged Care & Palliative Care consultant/educator
Jim Zubic
President of Orthodox Chaplaincy Association
Peter McHugh
Senior Pastor Christian City Church, Whitehorse
Persons in blue: Career is religion
Almost all of them are religious by career
To save you a lot of time assessing who these people are, I’ve coloured in blue all the folks whose job it is to espouse religion — at least, their own hierarchy’s view of it.
That’s 27 of the 29 signatories who by career are intensely immersed in their own religious perspective of the world; established and promoted through institutional doctrine.
But what about the other two?
What about the other two signatories, Assoc. Prof. Afif Hadi and Assoc. Prof. Rosalie Hudson (in yellow)?
Notice that Prof. Afif Hadi’s entry lists only his surgery profession. Highly relevant, but not mentioned, is that he was President (previously Vice Chairman) of the Australian and New Zealand Board of Trustees, Antiochian Orthodox Archdiocese of Australia and New Zealand. As head of the Board of the Archdiocese, his religious signature is intimately entwined with another: Metropolitan Archbishop Paul Saliba, the Primate of the Antiochian Orthodox Archdiocese.
Assoc. Prof. Rosalie Hudson’s listing too, mentions only seemingly secular links. What is omitted is that she is or was Chair of the University of Divinity (a multi-faith religious institution) Human Research Ethics Committee, Secretary of the Uniting Church’s committee on bioethics, a member of the Interfaith Committee, and an Academic Associate at Charles Sturt University’s School of Theology.
Thus, both Prof. Hadi and Assoc. Prof. Hudson are also deeply rooted in religious faith. The point is not to make any criticism of their faith or practice, but merely to observe the deeply religious connections to opposing assisted dying law reform. It’s worth mentioning that both Hadi and Hudson do valuable charity work.
So, all of them are deeply religious
A pertinent question to ask is: ‘What proportion of the signatories are neutral, scholarly researchers who have studied the empirical evidence from jurisdictions where assisted dying is already lawful?’ Answer: None of them. Enough said.
And what proportion of the signatories to this anti-assisted dying advertisement are very deeply invested in organised religion? The simple answer is as usual: 100%,all of them.
Disconnected from their flocks
Critically, these career-religious fail to reflect the views of their own flocks. We know from repeated polls, for example, that three out of four Australian Catholics, more than three out of four Uniting Church members, and four out of five Anglicans (Church of England) support assisted dying law reform.
This kind of clerical disconnect from the contemporary will of the people is one of the key reasons Australians are deserting religion in droves, as successive censuses show.
Conclusion
The evidence is irrefutable. Those who are actively organised to oppose your right to choose an assisted death are deeply religious, even when they use seemingly secular arguments (more on those later).
They are entitled to their opinions for themselves. But what right do they have to deny the vast majority of Australians, who do not agree with their views, the right to choose?
To phrase it in the personal, why does the Catholic Archbishop of Melbourrne, Denis Hart, think it appropriate to demand that Mr Geoff Drummond, a Buddhist, should have suffered against his will at the end of life for the Archbishop's version of faith, rather than Mr Drummond's own spiritual beliefs? Why does Rabbi Shimon Cowen think it appropriate to demand that Mr Alan Rosendorff, a fellow Jew, should have suffered against his will at the end of life for the Rabbi's version of faith, rather than Mr Rosendorff's own carefully-considered and deeply-held views? And why does Imam Riad Galil think it appropriate to demand that Mr Peter Short, not a Muslim, should have suffered against his will at the end of life for the Imam's beliefs, rather than his own?
Perhaps hubris remains alive and well amongst religious conservatives?
-----
Declaration: In fairness to those mentioned in this article, I openly declare that I am agnostic.
References
Bradbeer, G, Rt Rev., Carter, R, Rev., Champion, M, Rev. Dr, Conner, M, Pastor, Cooper-Clarke, D, Dr, Cowen, S, Rabbi Dr, Curlis-Gibson, M, Rev., Freier, P, Archbishop Dr, Galil, R, Imam, Grant SSC, J, Rev. Fr, Hadj, A, Assoc. Prof., Hart, D, Archbishop, Harvey, G, Rev. Fr, Hudson, R, Assoc. Prof., McHugh, P, Michell, GA, Rev. Fr, Nelson, G, Pastor, Palmer, D, Rev., Pietsch, G, Rev., Pietsch, M, Protopopov, M, Very Rev. Dr, Riordan, M, Saliba, P, Metropolitan Archbishop, Stasiuk, P, Bishop, Stephenson, D, Stevens, P, Pastor, Tonti-Filippini, N, Dr, Ward, R & Zubic, J 2008, Reject physician assisted dying - An open letter to Victorian MPs, Catholic Archdiocese of Melbourne, viewed 13 Jun 2008, http://www.cam.org.au/Euthanasia.aspx.
Blog by Neil FrancisPosted on Friday 2nd December 2016 at 5:34pm
The AMA announces an 'update' of its "euthanasia and physician assisted suicide" policy.
The Australian Medical Association (AMA) executive (policy group) recently concluded a major review of its official policy on assisted dying. The last major review was in 2007. Through a deeply flawed process the AMA executive continues to expressly disrespect the diversity of views amongst Australian doctors — a diversity confirmed by its own review — and hasn’t altered its opposition to assisted dying in any meaningful way.
Unrepresentative of Australian doctors
The AMA promotes itself as “leading Australia’s doctors,” yet more than two thirds of Australian doctors (70.5%) are not members. Its executive might like to think it’s leading, but most Australian doctors aren’t following. Claimed representation is particularly important when it comes to professional medical practice policies, because the AMA behaves as though its policies apply to all Australian doctors.
So who did the AMA consult in conducting its major review of policy on assisted dying? Only its own members. In other words, the AMA claims to represent all Australian doctors, but in reality consulted less than a third of them in the setting of its assisted dying policy. As AMA member Dr Rosemary Jones pointed out, some doctors eschew the AMA because of its opposed stance towards assisted dying. That creates a sampling bias in the AMA’s study… against assisted dying.
Further, the response rate to its survey of members was around 13%, meaning that only the most engaged AMA members (thus around 4% of all Australian doctors) offered a voice.
Biased survey
There are numerous flaws in the AMA’s survey. Here’s just one. In the preamble to the questionnaire, the AMA expressly told responding doctors (who, remember, are AMA members and probably don’t want to tick off their association) what its positions on certain end-of-life practices were. Then, in the first questions, it asked the doctor whether they agreed with the positions: strategies certain to result in substantial confirmation and acquiescence biases.
This just isn’t on. As a professional social and market researcher, I sent a detailed critique of the many problems with the survey to AMA President Dr Michael Gannon. I received a courteous but dismissive response from administration. A highly-respected Fellow of the Australian Market & Social Research Society sent a similar critique, also receiving a non-committal reply.
Survey results
While the AMA hasn’t published the survey results in detail yet, key headline statistics have been reported. What did the AMA discover on the basis of a methodology swayed against assisted dying?
Around four out of ten doctors believe that doctors should be involved in assisted dying cases, while around five out of ten thought they shouldn’t. One out of ten had no view either way.
If assisted dying were legalised, a majority said that doctors should be the ones to do this work.
That’s a clear message that a substantial proportion of doctors think assisted dying can not only be legitimate practice, but is the business of the medical profession — at least for those who wish to participate.
Executive’s ‘interpretation’
And what did the AMA executive make of these important insights after deliberating on them for months? Here are the AMA’s previous and ‘revised’ core policy statements:
Previous (2007) statement
‘Revised’ (2016) statement
“The AMA believes that medical practitioners should not be involved in interventions that have as their primary intention the ending of a person's life. This does not include the discontinuation of futile treatment.”
“The AMA believes that doctors should not be involved in interventions that have as their primary intention the ending of a person’s life. This does not include the discontinuation of treatments that are of no medical benefit to a dying patient.”
Despite the gratuitous change of a few words after a year of ‘research,’ the statement remains the same.
Doctors and the public have a right to ask of the AMA, “what part of the evidence that there is a genuine diversity of respectable views, did you miss?”
Failure to respect diversity
The executive might argue that it did listen. Here are its statements about diversity:
Previous (2007) statement
‘Revised’ (2016) statement
“The AMA recognises that there are divergent views regarding euthanasia and physician-assisted suicide.”
“The AMA recognises there are divergent views within the medical profession and the broader community in relation to euthanasia and physician assisted suicide.”
Despite another increase in wordiness, this statement too remains the same.
The AMA executive says it recognises that there are divergent views, but by continuing to insist that no doctor should be involved in assisted dying, it reveals that it doesn’t respect some views. How does it justify this hubris?
Failure to respect the patient
The revised policy also says in part:
“Doctors should … endeavour to uphold the patient’s values, preferences and goals of care.”
The sting in the policy tail is, given the AMA executive’s wholly opposed stance toward assisted dying, that the doctor should only uphold patient values, preferences and goals of care if the AMA executive approves of them (and assuming to do so is legal).
Was it a foregone conclusion?
The AMA executive’s continued opposition to assisted dying was unsurprising. The signals were clear. While the policy review was in play, AMA President Dr Michael Gannon made a series of tweets and media comments, all unsupportive of or directly opposed to assisted dying. Here’s a few.
In response to an article in The Australian “Catholic stance allows eased exit”, he tweeted a faux ‘competition’ between palliative care and assisted dying:
@amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian
He also tweeted in support of the ‘doctrine of double effect’, a controversial policy (which the AMA promotes as uncontroversial) that contends it’s quite OK for a doctor to hasten a patient’s death after all… provided they don’t really mean to: hardly a robust or verifiable standard.
@amapresident 24 Aug 2016: Doctors should be careful, must obey the law and understand their code of #ethics. Double effect is not #Euthanasia
In an article in The Australian on 15th September, Dr Gannon argued against assisted dying on the basis of it being ‘extremely complex.’ If complexity were a reason to oppose anything, the AMA would be opposed to the entire healthcare system: it’s incredibly complex. His argument collapses at the slightest inspection.
@amapresident 18 Sep 2016: Hippocratic medicine older than some of the world’s great religions, every political ideology, trend #ethics @medwma
Dr Gannon then invoked the Hippocratic Oath, which bans assisted dying. That’s cherry-picking at its best. Doctors do not take the Hippocratic Oath: it swears allegiance to ancient Greek gods, forbids women from entering the profession and outlaws surgery, amongst other things.
@amapresident 19 Sep 2016: Agree @DrSallyCockburn admire #euthanasia work done by @CMA_Docs. Equally careful, compassionate, intelligent approach from @TheBMA #ethics
He commends the British Medical Association’s “intelligent approach” against assisted dying: an approach I have comprehensively exposed as superficial and ill-informed fear-mongering, fiction, flip-flop and hubris.
@amapresident 1 Oct 2016: It is inevitable that if #Euthanasia laws are passed, they will over time be expanded to include children, mentally ill, vulnerable #ethic
Dr Gannon demonstrated ignorance of basic facts with this ‘slippery slope’ claim. In Oregon, which has the world’s oldest specific assisted dying framework (in effect since 1997), there have been no changes in who may qualify. He also ignores peer-reviewed research showing no ‘slippery slope’ for the supposed ‘vulnerable’. Canadian Professor Harvey Chochinov, Chair of his government’s expert panel which investigated legislative options for assisted dying, confirmed the evidential absence of the ‘slippery slope’ in a keynote address at Swinburne University in Melbourne last week.
@amapresident 11 Nov 2016: Doctors maintain this Trust with everyday care for patients, by upholding #DeclarationOfGeneva @medwma @juliamedew @Rania_Spooner #ethics
Dr Gannon also claimed that assisted dying would erode patient trust in doctors, at odds with the fact that people’s trust in doctors is high amongst OECD countries with assisted dying laws. Indeed, trust in doctors amongst Dutch, Belgian and Swiss citizens is significantly higher than Australians’ trust in our own doctors.
During the review period, Dr Gannon also repeatedly promoted the (medical) Declaration of Geneva (e.g. see previous tweet), which states that doctors must not participate in assisted dying. If the Declaration’s canonical opposition was indeed the authoritative stance on assisted dying, then it would be irrelevant for the AMA to conduct a review process of its policy.
Doctors and the public might ask a legitimate question: “Why did the AMA President think it appropriate to publicly and repeatedly indicate what review conclusion he favoured, while the review was in progress?”
Declining to correct misinformation
In September, the Medical Journal of Australia (MJA: a wholly-owned subsidiary of the AMA), published a news report containing significant misinformation that painted a hostile picture about assisted dying in Belgium. I published a critique of why the opinion was wrong, and commented on the online MJA article with a link to my correction. The MJA promptly deleted my comment.
AMA member Dr Rosemary Jones then put up the same objection which, by dint of her membership, they wouldn’t delete. The MJA then responded, but only to dig in its heels to defend the misinformation and reveal even more serious flaws in its arguments.
I wrote a further research-backed analysis of why its defensive arguments were even more wrong than the original and posted a note and link on the original MJA article page (Figure 1).
Figure 1: The second post on MJA inSight which was subsequently deleted.
Once again, my post has been deleted. The result of this is that erroneous information about Belgium remains published on the MJA website as though it is correct, while failing to mention or acknowledge that it has been soundly refuted.
It’s disappointing that the AMA and its President continue to make such uninformed remarks given that Dr Gannon claims to be a stickler for scientific evidence:
@amapresident 18 Aug 2016: Being a doctor is a huge privilege. Also carries responsibility to provide accurate scientific info, act ethically.
Spotlight on the AMA
Legitimate questions serve to shine a spotlight on the AMA. Firstly, given the circumstances, what was the likelihood of a real change to the AMA’s entrenched opposition toward doctor participation in assisted dying?
Secondly, given the AMA’s entrenched opposition, how can it expect its demands that it be consulted about any potential law reform to be treated seriously? If assisted dying is nothing to do with doctors, why is what doctors think relevant?
Utterly resistant to modernisation?
At its 2016 AGM, AMA member Dr Harry Hemley noted that the AMA largely represented its more hard-core, long-term older members and warned of the AMA’s increasing irrelevance and impotence (Figure 2). He moved an urgency motion to commission a review and report with “recommendations for a plan, vision and determination that will lead to re-invigorating and sustaining the AMA.”
Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform
The motion wasn’t in relation to an actual or particular reform: merely to investigate the potential for reform and to provide recommendations for consideration. We can only hope that the AMA will drag itself into the 21st century at some stage.
Conclusion
The AMA is deeply out of touch with Australians on the issue of assisted dying. It represents fewer than a third of Australian doctors and has failed to respect the very range of perspectives it obtained by consulting its members. It further strains its credibility by insisting that doctors mustn’t be involved in assisted dying, yet demanding to be consulted on any law reform to permit it.
If the AMA is to become relevant to contemporary society it must move on from the ‘old boy’ approach to medicine and adopt a stance of neutrality toward assisted dying. Only neutrality demonstrates appropriate respect for the true range of views held in good conscience by Australian doctors.
Fact file by Neil FrancisPosted on Sunday 13th November 2016 at 1:47am
Assisted dying rates in Dutch-speaking cultures (orange bars) are much higher than elsewhere.
In this whitepaper, Benelux (Belgium, Netherlands and Luxembourg) primary empirical data on assisted dying is analysed — including with new and advanced approaches — to provide fresh insights into contemporary practices. Investigation reveals that the assisted dying rate in Dutch-speaking cultures appears to be uniquely higher than in other cultures irrespective of the permissiveness of the legislative framework, yet is still practiced conservatively.
Download a full copy of the Whitepaper here: PDF (648Kb).
Summary
This new compilation and unique analysis of primary research data from statutory authorities and the peer-reviewed literature provides fresh insights into assisted dying practice in Benelux, including:
Rates of assisted dying in the Netherlands and Belgium have followed an expected sigmoid curve, now beginning to level out.
Several factors have contributed to the higher increase in the Netherlands rate, including recovery from a suppression of cases immediately following statutory reform, a rise in cancer diagnoses, and an increase in granting of assisted dying through new visiting teams launched in 2012.
Both Netherlands and Belgium doctors demonstrate caution if not conservatism when assessing assisted dying requests.
Despite most assisted dying occurring in cases of cancer, fewer than one in ten cancer deaths in the Netherlands and one in twenty in Belgium is an assisted death.
Other conditions such as degenerative neurological, pulmonary and circulatory illnesses each account for a very small proportion of the increase in cases since legalisation in Benelux.
The assisted dying rate in dementia and other mental illness is very low despite controversy around—and a tiny rise in granting of—such cases.
The hypothesis that females or the elderly would be ‘vulnerable’ to assisted dying law is contradicted by the data.
The rate of non-voluntary euthanasia has decreased significantly in both the Netherlands and Belgium since assisted dying was permitted by statute.
Assisted dying rates in Dutch-speaking cultures are significantly higher than in non-Dutch cultures, seemingly unrelated to the permissiveness of the jurisdiction’s legal framework.
Benelux country reported assisted dying rates (as a percentage of all deaths)
as at 2014. The three countries have similar assisted dying laws.
The F filesPosted on Friday 14th October 2016 at 1:21am
BMA House in Tavistock Square, London, home to the British Medical Association since 1925.
The British Medical Association (BMA), in the latest incarnation of its policy on assisted dying (AD), insists that AD must not be legalised in the UK. I argue that its indefensible stance reveals ignorance, incoherence and hubris. It fails to respect the true range of views amongst UK doctors. I expose the comprehensive rot.
The BMA categorically states in its July 2016 policy update on assisted dying:
“The BMA policy … insists that voluntary euthanasia [and] physician-assisted suicide should not be made legal in the UK.” — British Medical Association1
BMA comprehensively out of touch
The BMA claims to represent UK doctors—though fewer than half are members. What is the empirical evidence for UK doctor attitudes toward assisted dying?
In a 2009 survey,2 35% said that AD should definitely or probably be legalised. The same study also found that 35% of UK doctors said AD should definitely not be lawful even in cases of terminal illness. That is, the stance of just 35% of UK doctors was identical to the BMA’s—insisting that it not be lawful, while an equal proportion thought AD could be legalised. “Greater religiosity” was the strongest correlative factor with opposition to lawful AD.
Indeed, numerous studies have found a substantial minority of UK doctors in favour of lawful AD, including results approaching equality with opponents.3 Even a survey commissioned by the UK Catholic Medical Association in 2003 found around 25% of UK doctors in favour of AD and who would practice it if legalised.4
UK doctor support for AD, then, is substantial and hardly restricted to a mere handful of fringe-dwelling medical crackpots.
Ignorant and disrespectful BMA stance
It is untenable that the BMA unilaterally ‘respects’ the views of 35% of UK doctors at the same time as expressly disrespecting the views of another significant cohort. Perhaps as in general politics, its power base is more heavily populated with religious souls: those who have a deeper interest in shaping what options others do and don’t have?
Appalling and trivialised ‘rationale’
Let’s take a look at the five moribund reasons the BMA offers in defense of its institutional opposition to AD and see how they use flapdoodle, fudge, fiction, fear-mongering, flip-flop and hubris to ‘advance’ their position.
“Current BMA policy firmly opposes assisted dying for the following [five] key reasons:”
1. Permitting assisted dying for some could put vulnerable people at risk of harm.
Flapdoodle. Firstly, as I have explained before, the “vulnerable at risk” argument is a rhetorical sham. People ‘at risk’ are by definition ‘vulnerable,’ and would still be so if we wore yellow socks on Wednesdays or outlawed pizza. It has nothing to do with AD being legalised or not.
Fudge. Secondly, the BMA ignores repeated reviews published in the professional literature indicating that supposed harms have not eventuated in jurisdictions with lawful assisted dying. Indeed, the quality of medical practice has improved.
Flip-flop. And thirdly, if ‘risk of harm’ was a sufficient condition to deny patients a particular option, we must equally ban the right to refuse life-saving medical treatment (no matter how unwanted or burdensome) because greedy relatives eyeing off the estate might convince the dying patient to refuse. It’s incoherent to oppose assisted dying, but to support refusal of treatment (as the BMA does), in the face of this identical possibility.
2. Such a change would be contrary to the ethics of clinical practice, as the principal purpose of medicine is to improve patients’ quality of life, not to foreshorten it.
Fudge. Medicine has a number of primary purposes. Relief of suffering is one.5 That may come into conflict with another purpose, “the avoidance of premature death and the pursuit of a peaceful death” (which itself has internal conflicts). A dying individual may herself believe that an AD would not be premature, and whose peaceful nature is vastly preferable to continued intolerable and unrelievable suffering.
3. Legalising assisted dying could weaken society's prohibition on killing and undermine the safeguards against non-voluntary euthanasia. Society could embark on a 'slippery slope' with undesirable consequences.
Fear-mongering. Non-voluntary euthanasia (NVE) is currently illegal. It remains illegal even when AD is legalised. The BMA therefore incoherently conjectures that NVE doesn’t occur while it’s illegal (before AD legalisation), but might occur while it is still illegal (after AD legalisation).
Fiction. There are no current ‘safeguards’ against NVE as the BMA statement implies. It is practiced in secret. There are no statutory requirements or reporting standards as there are for AD (where legal). Research clearly demonstrates that NVE occurs everywhere, including the UK. Further, the rate of NVE has significantly decreased in the Netherlands and Belgium since their AD statutes came into effect.
4. For most patients, effective and high quality palliative care can effectively alleviate distressing symptoms associated with the dying process and allay patients' fears.
Flapdoodle. The BMA says “effective … palliative care can effectively alleviate…”: another circular, self-‘proving’ argument.
Hubris. The BMA acknowledges here—as unarguably established in the professional literature—that palliative care can’t help everyone. And that’s precisely what assisted dying law reform is about: for people that palliative care can’t help. But the BMA brushes them under the carpet.
5. Only a minority of people want to end their lives. The rules for the majority should not be changed to accommodate a small group.
Flip-flop. In ‘reasons’ 1 and 3 above, the BMA speculates that too many people will die if AD is legalised. Here is it arguing that too few will. Which is it? Too many or too few? The argument also ignores the international evidence that dying individuals (and their loved ones) experience profound relief merely from knowing that AD is available, even if they don’t pursue it. That itself is good palliative care.
Hubris. And if “not changing the majority's rules to accommodate a small group” were a gold standard as the BMA argues, then there would be no leglisation to (a) ensure facilities access to people with a disability, (b) outlaw discrimination on the basis of race or religion, or (c) allow same-sex marriage: all enshrined in law in the UK.
Hubris argues for ignoring the BMA itself
If, as the BMA argues, we should override the wishes of a group on the basis of its small size, it’s pertinent to consider the size of the UK doctor population: around 0.4% of the total. By comparison, in jurisdictions where AD is legal, around 0.3% (Oregon) to 3.8% (Netherlands) ultimately choose an assisted death.
If we are to ignore 0.3%–3.8% of the population because it’s ‘too small,’ we must equally ignore 0.4% of it. This, by the BMA’s own argument, would be reason to force it to support AD because that’s what the majority (UK population) favour. After all, “the rules for the majority should not be changed to accommodate a small group [of doctors].”
Of course most of us recognise, unlike the BMA, that this is not a ‘popularity contest.’ A stance of neutrality would demonstrate respect for deeply-held views across the spectrum.
Conclusion
The British Medical Association demonstrates profound ignorance about the available evidence, and about UK doctor attitudes. It resorts to fear-mongering speculation, fudge, fiction, flapdoodle, flip-flop and hubris to maintain its indefensible opposition to assisted dying.
The BMA’s stance does a great disservice to the British people. It’s an embarrassment to professional doctors regardless of their stance on assisted dying. The policy deserves to be entirely scrapped, and one of neutrality adopted in its place.
Seale, C 2009, 'Legalisation of euthanasia or physician-assisted suicide: survey of doctors' attitudes', Palliative Medicine, 23(3), Apr, pp. 205-212.
McCormack, R, Clifford, M & Conroy, M 2011, 'Attitudes of UK doctors towards euthanasia and physician-assisted suicide: a systematic literature review', Palliative Medicine, 26(1), pp. 23-33.
Catholic Medical Quarterly 2003, 'Euthanasia and assisted suicide: Results of survey of doctors attitudes', Catholic Medical Quarterly, May, pp. 1-3.
Hastings Center Report 1996, 'The goals of medicine. Setting new priorities', The Hastings Center Report, 26(6), pp. S1-27.
Blog by Neil FrancisPosted on Saturday 24th September 2016 at 11:31pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
Against current moves to legalise assisted dying, Australian Catholic Father John George invokes Nazi Germany, resorts to ad hominem attacks to dismiss those who disagree with him, and demands that the Pope’s edicts are binding on everyone regardless of their own faith or world view.
On 24th September 2016, Journalists Greg Brown and Rick Morton published an article in The Australian, Victorian coroner credited with turning tide on euthanasia, summarising recent Australian moves to legalise assisted dying choice.
Catholic Father John George commented on the article online, quoting four sections of the Catholic Church’s catechism that prohibit assisted dying (sections 2276–9).
Pushback
Other readers of The Australian remarked that they respected his view for himself but they had no interest in the Pope’s views given the readers were not Catholic. In fact, repeated polls in Australia have shown that even the great majority of Catholics (three out of four) do not agree with the Vatican on the matter of assisted dying, a matter which Fr George dismisses merely as ‘fickle votes and polls.’
I would remind Fr George that these are not fickle: Australian public opinion in favour of assisted dying choice has been consistently in the majority for now more than four decades.
Fr George further quoted Catholic sources, for example the LJ Goody Bioethics Centre in Perth, Australia, which he failed to mention is, literally, an agency of the Catholic Archdiocese of Perth. He also selectively quoted Palliative Care Australia, failing to mention that they have acknowledged that not all pain and suffering can be eliminated at the end of life, even with the best palliative care.
Ad hominem attack
In response to a rising tide of objections to his musings, including from Mr Ian Wood, a fellow Christian and co-founder of Christians for Voluntary Euthanasia Choice, Fr George resorted to the ad hominem attack: to attack the person (or persons) rather than the arguments. He said:
“The pro euthanasia claque here make professional Nazi propaganda expert Goebbels look like a 5th rate amateur.” — Father John George.
For anyone in the dark, a claque is a group of sycophants hired to applaud a performer or public speaker. How rude. Fr George seems to have neglected to reflect that it is he who is hired to promote the performance of the Vatican. I applaud his right to do so, and I do not compare him to a treacherous propagandist in a murderous wartime regime in order to dismiss his arguments: I address the arguments themselves.
Nazi Germany
Fr George makes repeated mentions of Nazi Germany as a core reason to deny assisted dying choice.
In contrast, several years ago I was chatting at a conference with the pleasant and engaging Peter McArdle, then Research Director of the Australian Catholic Bishop’s Conference. He volunteered that he very much disliked the “Nazi Germany” argument so often used in religious circles, and wished it would stop because in so doing it meant they’d already lost the debate.
I agree. It’s a lazy and indefensible argument: that rational people in a functioning democracy must be denied choice for themselves on the basis of what some murderous regime did against others at the point of a gun.
Indeed, to rely on such a standard would be to equally argue against the right to religious practice, because the Catholic Church, through its inquisition practices (medieval C12th, papal C13th, Spanish C15th, Roman and Portuguese C16th) relied on torture and resulted in confiscation of property and at least tens (if not hundreds) of thousands of executions for witchcraft and heresy.
Ultimate hubris
But the real crux is that Fr George then unequivocally demands that:
“Principles elaborated by the pope are universally applicable.” — Father John George.
This ultimate hubris reveals a profound lack of self-reflection, both personally and organisationally. Even entertaining for a moment the premise that one individual (or even organisation) can tell everyone on the planet how they must live their lives, how would we choose that person or organisation? Why is it less valid for the head of any other branch of Christianity, of Judaism, Islam, Hinduism, Buddhism (or any other religion) or an agnostic (which I am) or an atheist, to set such rules for everyone, overriding other deeply-held beliefs and values?
A keener example of ‘blinded by faith’ would be hard to find.
Conclusion
I argue that Fr John George displays some of the gravest hubris of some members of the Catholic church. I respect and applaud his world views for himself and those who wish to subscribe. But using canonincal arguments (that is, religious arguments demanded as universally true by virtue of the supposed authority that dispensed them) is probably a major contributor to the current flight of people away from organised religion.
More happily, such an attitude is also contributing to accelerating the legalisation of assisted dying choice because folks can see these arguments for what they are. For that I doff my hat to Fr George.


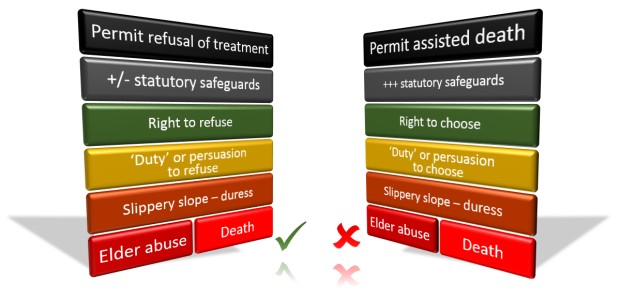 The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.

 Infographic summary of 'AMA uncovered'
Infographic summary of 'AMA uncovered'

 @amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian
@amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian Figure 1: The second post on
Figure 1: The second post on  Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform
Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform