Blog by Neil FrancisPosted on Saturday 24th September 2016 at 11:31pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
Against current moves to legalise assisted dying, Australian Catholic Father John George invokes Nazi Germany, resorts to ad hominem attacks to dismiss those who disagree with him, and demands that the Pope’s edicts are binding on everyone regardless of their own faith or world view.
On 24th September 2016, Journalists Greg Brown and Rick Morton published an article in The Australian, Victorian coroner credited with turning tide on euthanasia, summarising recent Australian moves to legalise assisted dying choice.
Catholic Father John George commented on the article online, quoting four sections of the Catholic Church’s catechism that prohibit assisted dying (sections 2276–9).
Pushback
Other readers of The Australian remarked that they respected his view for himself but they had no interest in the Pope’s views given the readers were not Catholic. In fact, repeated polls in Australia have shown that even the great majority of Catholics (three out of four) do not agree with the Vatican on the matter of assisted dying, a matter which Fr George dismisses merely as ‘fickle votes and polls.’
I would remind Fr George that these are not fickle: Australian public opinion in favour of assisted dying choice has been consistently in the majority for now more than four decades.
Fr George further quoted Catholic sources, for example the LJ Goody Bioethics Centre in Perth, Australia, which he failed to mention is, literally, an agency of the Catholic Archdiocese of Perth. He also selectively quoted Palliative Care Australia, failing to mention that they have acknowledged that not all pain and suffering can be eliminated at the end of life, even with the best palliative care.
Ad hominem attack
In response to a rising tide of objections to his musings, including from Mr Ian Wood, a fellow Christian and co-founder of Christians for Voluntary Euthanasia Choice, Fr George resorted to the ad hominem attack: to attack the person (or persons) rather than the arguments. He said:
“The pro euthanasia claque here make professional Nazi propaganda expert Goebbels look like a 5th rate amateur.” — Father John George.
For anyone in the dark, a claque is a group of sycophants hired to applaud a performer or public speaker. How rude. Fr George seems to have neglected to reflect that it is he who is hired to promote the performance of the Vatican. I applaud his right to do so, and I do not compare him to a treacherous propagandist in a murderous wartime regime in order to dismiss his arguments: I address the arguments themselves.
Nazi Germany
Fr George makes repeated mentions of Nazi Germany as a core reason to deny assisted dying choice.
In contrast, several years ago I was chatting at a conference with the pleasant and engaging Peter McArdle, then Research Director of the Australian Catholic Bishop’s Conference. He volunteered that he very much disliked the “Nazi Germany” argument so often used in religious circles, and wished it would stop because in so doing it meant they’d already lost the debate.
I agree. It’s a lazy and indefensible argument: that rational people in a functioning democracy must be denied choice for themselves on the basis of what some murderous regime did against others at the point of a gun.
Indeed, to rely on such a standard would be to equally argue against the right to religious practice, because the Catholic Church, through its inquisition practices (medieval C12th, papal C13th, Spanish C15th, Roman and Portuguese C16th) relied on torture and resulted in confiscation of property and at least tens (if not hundreds) of thousands of executions for witchcraft and heresy.
Ultimate hubris
But the real crux is that Fr George then unequivocally demands that:
“Principles elaborated by the pope are universally applicable.” — Father John George.
This ultimate hubris reveals a profound lack of self-reflection, both personally and organisationally. Even entertaining for a moment the premise that one individual (or even organisation) can tell everyone on the planet how they must live their lives, how would we choose that person or organisation? Why is it less valid for the head of any other branch of Christianity, of Judaism, Islam, Hinduism, Buddhism (or any other religion) or an agnostic (which I am) or an atheist, to set such rules for everyone, overriding other deeply-held beliefs and values?
A keener example of ‘blinded by faith’ would be hard to find.
Conclusion
I argue that Fr John George displays some of the gravest hubris of some members of the Catholic church. I respect and applaud his world views for himself and those who wish to subscribe. But using canonincal arguments (that is, religious arguments demanded as universally true by virtue of the supposed authority that dispensed them) is probably a major contributor to the current flight of people away from organised religion.
More happily, such an attitude is also contributing to accelerating the legalisation of assisted dying choice because folks can see these arguments for what they are. For that I doff my hat to Fr George.
Blog by Neil FrancisPosted on Sunday 28th August 2016 at 12:58am
Brad Mattes' blog containing misleading and evidentially false statements.
The latest misinformation employed by assisted dying opponents is to imply that Belgium’s general suicide rate is high as a consequence of its assisted dying law: i.e. to argue the discredited 'suicide contagion' line which has in the past been peddled about the USA state of Oregon. I have demonstrated that it was false in Oregon, and I equally demonstrate here that it's false in Belgium.
Mr Brad Mattes recently published emotional anti-assisted-dying nonsense in LifeSiteNews. (LifeSiteNews is a Canadian blog site that was established by the conservative Christian Campaign for Life Coalition and which has a primary principle of promoting “traditional Judeo-Christian principles”. Mr Mattes is radio host for Ohio’s Life Issues Institute, an anti-abortion lobby group established by conservative American John C. Willke who claimed that women’s bodies were resistant to pregnancy as a result of rape.)
Putting on the misinformation running shoes
In his blog Mr Mattes quickly establishes a practice of communicating misinformation by first claiming that assisted dying laws have “devastating effects” around the world including Japan and Albania—which don’t have such laws.
He then sprints onwards to the ‘650 babies euthanized in the Netherlands’ claim—which I have already comprehensively exposed as fake in the Journal of Assisted Dying—and then onto the bogus claim that the Netherlands has descended into a mire of ‘killing’ without the patient’s ‘consent,’ contrary to empirical evidence I've published that such actions occur around the world regardless of assisted dying laws, and which have decreased significantly in the Netherlands and Belgium since their assisted dying statutes came into effect in 2002.
Let’s add fries to that
Having served up a lot of fat and salt that might appeal to those on a fast-food anti-assisted-dying diet, he then offers the unqualified statement:
“By the way, Belgium has the second-highest suicide rate (nonrelated to euthanasia) in Western Europe.” — Brad Mattes
The ‘informational’ consequence is unequivocal: by Mr Mattes failing to contextualise this ‘incidental factoid’ in any way, the reader is destined to deduce that it is Belgium’s euthanasia law that causes Belgium’s suicide rate to be the second-highest in Western Europe. In other words, Mr Mattes is another poorly-informed commentator using the 'suicide contagion' line.
But what are the facts?
Depending on the source and year of data, one can certainly argue that Belgium’s general suicide rate is the second-highest in Western Europe. Setting aside for now the serious question of why it is valid to exclude all of the world’s other countries from the comparison, WorldLifeExpectancy.com reports figures that were published in 2014 (Table 1).
Table 1
Country
Suicides*
Finland
15.11
Belgium
14.64
Iceland
14.06
France
12.84
Austria
11.87
Sweden
11.43
Ireland
11.06
Germany
9.59
Switzerland
9.56
Norway
9.28
Denmark
9.19
Luxembourg
9.14
Netherlands
8.54
Portugal
8.49
Turkey
7.92
UK
6.28
Malta
5.75
Spain
5.23
Italy
4.76
Greece
3.86
* Suicides per 100k population, age-adjusted
The table includes all the countries in the wider definition of “Western Europe”, bar four: no suicide statistics are published for Liechtenstein, Monaco, Andorra or San Marino.
As you can see, Belgium is indeed the second-highest. But this begs the question:
If the reason Belgium is the second-highest is due to its assisted dying law, how come Finland, which Mr Mattes doesn't mention by name and which has no such law, is higher?
It also begs the question:
If assisted dying law were the fundamental cause of a high general suicide rate, how come Switzerland (statute since 1942), Luxembourg (statute since 2009) and the Netherlands (practice since the early 1980s and statute since 2002) have rates that are muchlower, all key facts that Mr Mattes also fails to mention?
These are of course indications that the factoid has been included as a cherry-picked morsel of 'proof' because it sounds so compelling as a throw-away sentence amongst the other (false) statements.
But wait, there’s more
We can go further than merely wondering about the country comparisons, by comparing Belgium’s general suicide rate before and after assisted dying law reform. A critical step in establishing causation is to first establish correlation. If there is no correlation, there can be no causation.
Published OECD data shows that in 2013 (the most recent available data), Belgium’s general suicide rate was 16.7 per 100,000 population. What was it before their 2002 law reform? Well in 2000 it was 20.5, in 1990 it was 19.2, … you get the idea.
Has Belgium’s general suicide rate soared (or even increased modestly) since their 2002 assisted dying law came into effect? No. It’s dropped. Indeed, the slight downward trend apparent before the statute came into effect in 2002 has accelerated downward since (Figure 1).
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Even the headline is misleading
Mr Mattes fails to point out in his blog that assisted dying statutes in Benelux countries (Belgium, the Netherlands and Luxembourg) never restricted access to only the 'terminally ill,' that is, those imminently dying. He also fails to point out that USA states whose laws do restrict assisted dying to the terminally ill—most notably Oregon and Washington—have not changed their statutes in this regard since they came into effect.
Therefore, his headling implying that lawful jurisdictions have broadened their laws from 'only the terminally ill' is also wrong.
Conclusion
Mr Mattes makes multiple false and misleading claims and it’s easy to see his opinion for what it is: an emotional dump that fails to engage with and indeed flies in the face of actual evidence. The latest 'suicide contagion' implication, that assisted dying law causes Belgium’s general suicide rate to be the “second-highest in Western Europe” is evidentially false.
I call on LifeSiteNews to withdraw Mr Mattes' article because it breaches their primary principle:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.” — LifeSiteNews
Summary of facts
Belgium's general suicide rate is one of the higher ones in Western Europe. However:
At least one country without an assisted dying law has a higher suicide rate, inconsistent with 'suicide contagion' theory.
Other Western Europe countries with assisted dying laws have suicide rates much lower than Belgium's, also at odds with 'suicide contagion' theory.
But the clincher is that the suicide rate in Belgium has dropped, not risen, since their 2002 assisted dying law came into effect.
Fact file by Neil FrancisPosted on Thursday 7th July 2016 at 10:19pm
Lead author Professor Ezekiel Emanuel discusses the findings of the JAMA study.
Several of the world's foremost researchers in medical end-of-life matters have released a detailed and comprehensive review of the practice of assisted dying in lawful jurisdictions around the world. Published in the Journal of the American Medical Association, it does not support slippery slope hypotheses.
Professors from universities in the USA, the Netherlands and Belgium studied data from government and statutory authority reports, primary scientific studies and other sources to examine how assisted dying has been practiced in different jurisdictions around the world where it is lawful in one form or another: self-administered medication (physician-assisted dying) or physician-administered medication (active voluntary euthanasia).1
Their primary conclusion is that:
"Euthanasia and physician-assisted suicide are increasingly being legalized, remain relatively rare, and primarily involve patients with cancer. Existing data do not indicate widespread abuse of these practices."
Key findings
Key findings include:
Public opinion favouring assisted dying in developed countries has been increasing, or remained stable at high levels of approval.
The trends seem to correlate with decreasing religiosity in Western countries.
The only place where assisted dying approval appears to be decreasing is in eastern Europe, where religiosity has been increasing.
Approval amongst physicians seems to be consistently lower than amongst the public.
Assisted dying occurs everywhere, including juridictions where it is unlawful (as I have previously reported).
Most individuals who choose assisted dying have advanced cancer (as I have previously reported).
Supposedly 'vulnerable' groups are not represented in assisted dying figures at rates any higher than their presence in the overall population.
Numbers of assisted deaths in lawful jurisdictions continue to increase, but represent a tiny minority of deaths.
In jurisdictions where only self-administration is permitted, assisted deaths represent around 0.3% of all deaths.
In jurisdictions where physicians may administer, assisted deaths represent around 3–5% of all deaths.
Assisted deaths for minors and those with dementia are a very small minority of cases (as I have previously reported).
The dominant reasons for requesting assisted death include loss of autonomy and dignity and the inability to enjoy life and regular activities; not physical pain.
Doctors still report that honouring a request for assisted death is emotionally burdensome; not a routine or welcomed option.
"In no jurisdiction was there evidence that vulnerable patients have been receiving euthanasia or physician-assisted suicide at rates higher than those in the general population."
Complication rates
One aspect of the study is worthy of special mention: the small rate of assisted dying procedure complications. The available data suggests that complications may occur more often for self-administered medication than for physician administration:
For self-administration—
Difficulty in swallowing in 9.6% of cases
Vomiting or seizures in 8.8% of cases
Awakening from coma in 12.3% of cases
For physician administration—
Technical problems such as difficulty in finding a suitable vein in 4.5% of cases
Vomiting or seizures in 3.7% of cases
Awakening from coma in 0.9% of cases
This data is however of Dutch practice in the 1990s, before assisted dying was codified in statute—at a time when practice was poorly defined and a range of drugs, including opioids, were widely used. Now, practice is well-defined with almost universal use of barbiturates. The researchers expressly note that these complication rates may well have reduced.
Further, the authors refer to more recent data from Oregon and Washington which indicate very much lower complication rates (in those jurisdictions for self-administration only):
In Oregon, the complication rates are around 2.4% for regurgitation and 0.7% for awakening from coma.
In Washington, the complication rates are around 1.4% for regurgitation, plus a single case of seizure.
The importance of context
It is worth comparing the complication rates of assisted dying procedures with rates for other medical interventions to provide an appropriate context so that they may be realistically interpreted.
For example, a study of common over-the-counter analgesics for short-term pain management2 found that significant adverse effects occurred amongst 13.7% of ibuprofen users, 14.5% of paracetamol useres and 18.7% of aspirin users.
In another example, an anlaysis of primary research about surgical outcomes found that 14.4% had adverse events, almost half of which (47.5%) were moderate to fatal in severity.3
Conclusion
The study is a solid synthesis of research data and indicates that assisted dying is accessed sparingly and in accordance with the intentions of each legislature.
The adverse event rate for assisted dying appears to be substantially lower than the rate of adverse events in the use of common over-the-counter analgesics and in surgery.
References
Emanuel, EJ, Onwuteaka-Philipsen, BD, Urwin, JW & Cohen, J 2016, 'Attitudes and practices of euthanasia and physician-assisted suicide in the united states, canada, and europe', JAMA, 316(1), pp. 79-90.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
Anderson, O, Davis, R, Hanna, GB & Vincent, CA 2013, 'Surgical adverse events: a systematic review', Am J Surg, 206(2), pp. 253-62.
Blog by Neil FrancisPosted on Thursday 12th May 2016 at 4:30pm
The more anti-euthanasia campaigner Mr Wesley Smith publishes, the more I think he’s missed his true vocation as a comedian. His latest comical gig against assisted dying is a gem.
Mr Smith starts with the case of two Californian doctors found guilty of Medicare fraud: billing fake hospice care for patients who weren't terminally ill. He artfully turns the story into a series of anti-assisted-dying gags.
Who’s on first, What’s on second?
Mr Smith directly connects the money-grabbing fraud case with the Obama administration, ribbing us that the President and federal authorities won’t hold doctors accountable for breaking assisted suicide law. Mr Smith, an attorney, is holding his breath to see if his audience figures out this little joke: oh, the confused jurisdiction names… right!
The Death With Dignity laws are State laws. If the law is broken it is State responsibility to pursue and prosecute offenders. The Feds have no jurisdiction. If, however, Medicare has been defrauded then it’s a Federal matter (FBI): and the Feds did indeed investigate and prosecute.
It’s a bit like the Laurel and Hardy confused “Who’s on first, What’s on second” name sketch, isn’t it? But only if you get it. Grin.
I say, I say, I say: what’s worse—being evil or being dead?
Mr Smith then refers to the case of Michael Freeland, an Oregonian dying of lung cancer who considered using the Death With Dignity Act. Citing himself and referring to the physician who prescribed lethal medication, Mr Smith compares Dr Peter Reagan with the Medicare fraudsters, saying that Dr Reagan “regularly takes on patients solely for the purpose of facilitating their suicides.”
Defamation is always good for a cackle. It’s so droll, like saying that Mr Smith “opposes assisted dying solely because of the great value of redemptive suffering whether others agree or not.” Which, of course, your dear writer is not saying (because Mr Smith has already stated on the record that he doesn't think suffering is redemptive).I’m just saying, you know, for laughs.
Wesley Smith jokes that Dr Peter Reagan is both evil and dead.
To add even greater mirth, Mr Smith describes Dr Reagan as “now late”. OMG, I've met Dr Reagan and he’s a top fellow. He’s died!? No, he hasn't. Fortunately, like Mark Twain, Dr Reagan happily reports that news of his death has been greatly exaggerated.
Phew, comic relief—what a hoot.
The Clause you have when you’re not having a Clause
Mr Smith then tells the one about how doctors ordinarily have to comply with an accepted medical “standard of care,” but that “death doctors” (love those stereotypes, chuckle!) only have to act in “good faith,” which, Mr Smith razzes us, is quite hard to assess. Oh. Awkward audience silence; a cricket chirps. Um, punchline please?
You have to supply your own punchline for this quip I’m afraid, because Mr Smith rather absent-mindedly forgets to. The Oregon Death With Dignity Act 1997 says explicitly in Clause 126.885 §4.01(7), “No provision [of this Act] shall be construed to allow a lower standard of care…”
Ah, more comic relief: the old 'pull-the-wool-over-your-eyes' caper, chortle.
The flip-flop routine
But the most comical gag is the one I reckon Mr Smith doesn’t even realise he’s told: the joke that we’re all going to die from lethal prescriptions, artfully developed by featuring someone he carefully points out didn’t take the lethal prescription. We just love a good flip-flop. LOL.
Oh, that and teasing us that the Medicare fraud case in which the purpose was to get more money is a great story against assisted dying whose purpose, he banters, is to get less (save) money. Double flip-flop: Ta-ching!
Blog by Neil FrancisPosted on Tuesday 8th March 2016 at 7:53pm
Dr Syme consults with Mr Bernard Erica (ABC Australian Story)
Australia's Medical Registration Board (AHPRA) has told Dr Rodney Syme that he is a serious danger to patients.
Dr Rodney Syme, who occasionally provides advice and medication for dying patients to give them control over their dying process, has been reprimanded by Australia's Medical Registration Board (AHPRA) for posing a 'serious danger' to such patients. The story has been reported widely in the media.
On ABC's Australian Story on Monday night, "My conscience tells me", patient Mr Bernard Erica clearly volunteers that this is utter nonsense, and that like former journalist Mr Steve Guest, who Dr Syme also provided advice and medication to control the end of his life, Mr Erica in no way felt Dr Syme was a threat of any kind. Indeed, like Mr Guest, he has experienced profound and lasting relief from the very knowledge he would have control if and when the time for him came.
Mr Erica's GP, who was aware of and seemed initially supportive of Mr Erica's stance and Dr Syme's advice and medication, lodged a complaint with AHPRA when the ABC's Australian Story contacted him (the GP) for an interview in relation to the case, it was explained on Australian Story. Did this doctor suddenly feel frightened into 'protecting his own arse'?
Coroner's Court data shows that 8.5% of suicides in Victoria are the result of dying patients in extremis being denied the right to a peaceful, doctor-assisted death.
AHPRA need to hear from ordinary Australians, and doctors, that they disagree with the stance it has taken in relation to Dr Syme's careful and compassionate consultations with dying patients. Indeed, to oppose careful and considered medical assessment that providing control is the only way for this particular patient to obtain relief from intolerable psychological suffering—of the State's refusal to allow rational and deeply valued paths to death—is to condemn such patients to a high chance of violent and undignified suicide.
In a key submission to the Victorian Parliament's current inquiry into end-of-life choices, the Coroner's Court of Victoria reported that, after intensive and exquisitely careful analysis, rejecting any equivocal cases, 8.5% of suicides in Victoria are of dying persons experiencing unrelievable and intolerable suffering, and for whom current law does not provide a compassionate and peaceful doctor-assisted death.
By censuring doctors who provide patient choice, it is my view that AHPRA becomes complicit in violent suicides amongst the terminally ill. Thus it is AHPRA and not Dr Syme who represents a 'serious danger' to terminally ill patients.
By reprimanding Dr Syme for his careful and considered private medical practice and for placing additional conditions on his medical license, it is my view that AHPRA becomes complicit in violent suicides amongst the terminally ill. Thus it is AHPRA and not Dr Syme who represents a 'serious danger' to terminally ill patients.
I wrote to AHPRA to express my displeasure at their failure to recognise contemporary community standards, which are enormously in favour of providing terminally ill people the right to a peaceful, doctor-assisted death. Here is what I said.
Dear AHPRA,
I write to express my dismay, along with millions of Australians, at your hostile attitude towards Dr Rodney Syme and your farcical claim that he is a danger to patients. Clearly, you are mired in nineteenth century medical paternalism and are out of touch with contemporary Australian attitudes about having control over one's death in the face of intolerable and unrelievable end-of-life suffering.
Dr Syme will speak for himself of course. But I will also say that having worked with Dr Syme for years, NEVER ONCE in my experience has his "primary intention " (as you put it) been for his patient to end their life when he provides advice and medication. He provides GOOD PALLIATIVE CARE: relieving intolerable psychological suffering. Many of his patients never take the medication.
Please lift your game and modernise. Dr Syme is giving patients control to live better, not inciting them to die: a choice between ways of dying, not between living and dying.
Neil Francis
I urge you to write to AHPRA as well, which you can do here. Scroll down the page to use the web form.
Blog by Neil FrancisPosted on Saturday 2nd January 2016 at 12:35am
Dr William Toffler (left) acknowledges no slippery slope cause-and-effect evidence, with Drs Bentz and Stevens
A new scholarly journal focused on end-of-life ethics, decision-making and practice has just been launched: the Journal of Assisted Dying. In the first article, claims by Oregon lobby group Physicians for Compassionate Care (PCC), including Doctors Bill (William) Toffler and Ken Stevens (and others) are assessed against empirical evidence and found to be completely wrong, or highly misleading as a result of selective use of data.
The new scholarly journal, the Journal of Assisted Dying, is dedicated to careful and holistic analysis of evidence in regard to the various forms of assisted dying that are lawful in a number of jurisdictions around the world... and to practices in jurisdictions where assisted dying remains illegal.
In the first article of a series on Oregon, I examine claims and speculations made by various doctors (and others who quote them), that Oregon has the second-highest suicide rate in the USA (or is always in the top 10), that Oregon's Death With Dignity Act has resulted a massive increase in the state's general suicide rate, and other astonishing statements.
Of course, the empirical evidence from the Oregon Health Authority and from the USA Centers for Disease Control and Prevention does not support these statements and interpretations, and I analyse and critique the evidence.
Some of the claims are just plain factually and hugely wrong. Others are the result of failing to read their sources more carefully, misunderstanding what the data actually represents. Still further claims are made on the basis of selectively-chosen statements from government reports, while omitting statements that are contrary to, or provide alternative and well-researched explanations for Oregon's recently rising general suicide rate.
Drs Toffler and Stevens have even published some of their claims and speculations in the British Medical Journal.1 It goes to show that even good journals sometimes publish bunkum: their article was a letter to the editor rather than peer-reviewed research. Great care is required to sort real evidence from hype and opinion.
Ultimately, Dr Bill Toffler of PCC has acknowledged on video that there is no cause-and-effect evidence between Oregon's Death With Dignity Act and Oregon's suicide rate, an acknowledgement that went unchallenged by his two PCC colleagues present at the time, Dr Ken Stevens and Dr Chuck (Charles) Bentz. You can see Dr Toffler's statement here (at 10'50").
The Journal of Assisted Dying is an open-access journal, and you can read the full article here.
-----
1. Toffler, WL & Stevens, K 2015, 'Re: Assisted dying: law and practice around the world', BMJ, vol. 351, 19 Aug, p. h4481.
Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 1–6.
Abstract
Background: Several physicians have speculated that Oregon’s general suicide rate is evidence of suicide contagion as a result of Oregon’s Death With Dignity Act (‘the Act’). Methods: Search and analysis of physician and related online sources of Oregon suicide contagion speculation; retrieval and analysis of cited Centers for Disease Control and Prevention (CDC) and other publications relied upon; analysis of authoritative, public Government mortality data for Oregon and other USA states. Results: Several physicians have speculated about Oregon suicide statistics in a manner that is not supported by the cited publications, or by public CDC mortality database data. The claims variously (a) misrepresent key data in the publications, (b) omit information in the publications that is at variance with suicide contagion speculation, and (c) overlook other significant information at variance with speculation. The physicians have previously acknowledged inability to prove perceived “slippery slope” effects of the Act. Other opponents of the Act have republished the physicians’ erroneous information. Conclusions: Evidence advanced by several physicians to speculate that Oregon’s Death With Dignity Act causes suicide contagion in Oregon is variously false, misleading or highly selective—omitting key facts—and has arisen even though the physicians acknowledge they have no proof of ‘slippery slope’ effects.
Article keywords
suicide contagion, copycat suicide, Werther effect, slippery slope, misinformation, Oregon, Dr William Toffler, Dr Kenneth Stevens, Physicians for Compassionate Care
Full PDF
Download the full PDF: (390Kb)
Citation
Francis, N 2016, 'Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon', Journal of Assisted Dying, vol. 1, no. 1, pp. 1-6.
Blog by Neil FrancisPosted on Wednesday 25th November 2015 at 8:00pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
On Wednesday 19th November 2015, the Catholic Church appeared before the Victorian Parliament's Legal and Social Issues Committee. Monsignor Anthony Ireland, the Episcopal Vicar for Health, Aged and Disability Care, and Father Anthony Kerin, Episcopal Vicar for Life, Marriage and Family gave evidence about end-of-life decision making. They made a factually wrong allegation about Oregon during their testimony.
Anthony Ireland spoke first, making it clear that they were appearing before the Committee with delegated authority from the Catholic Archbishop of Melbourne (Denis Hart) and with the endorsement of the Victorian Catholic Bishops. He emphasised that "the Catholic Archdiocese of Melbourne does not come to this Committee with fanciful or frivolous arguments."
During question time. Committee Chair Edward O'Donohue asked the Vicars if they had any evidence from lawful jurisdictions to back up their claim that legalising assisted dying would result in a significant reduction in medical research. The Vicars flailed about with vague hypotheticals, but no evidence.
Committee Deputy Chair Nina Springle remarked that some of their testimony was inconsistent with direct evidence from lawful jurisdictions and invited them to reflect on the contradictions. To this, Anthony Kerin stated:
"We know, for example, since Oregon legislated, that the standard suicide rate has increased remarkably and alarmingly. It's not yet the largest rate in the US, but it's getting there, when Oregon had a very, very low suicide rate prior to that."
Let's not mince words: the allegation is comprehensively false. In fact it's three false statements all wrapped up into one.
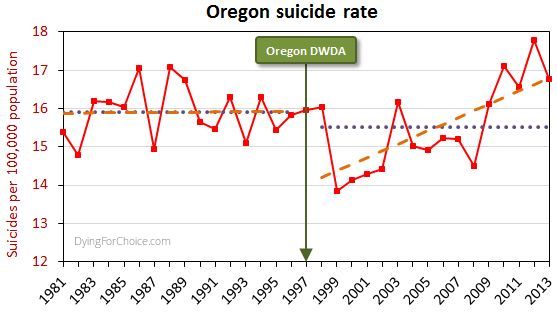
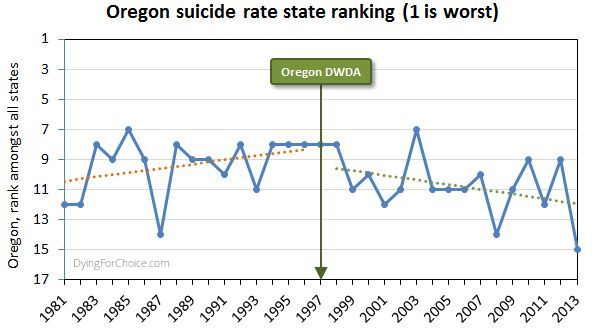
The USA government's CDC mortaility database provides solid empirical data. Here's Oregon's longitudinal suicide rate statistics, including sixteen years before its Death With Dignity Act (DWDA), and sixteen years after.
Here are the pertinent facts about Oregon's general suicide rate:
The average for the 16 years after the DWDA is lower than, but not statistically different from, the 16 years prior to the Act.
There was a massive drop in the suicide rate two years after the DWDA came into effect, and the rate has risen only from there.
The rise from 2000 onwards is repeated in the majority of USA states and in the national average. The trend increase in Oregon is not statistically different from the national trend increase.
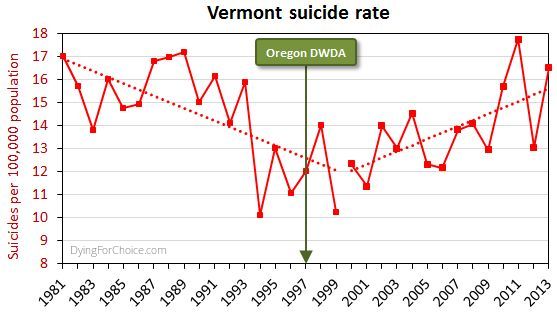
By way of comparison, here's Vermont's suicide rate for the same period.
Now, Vermont didn't have an assisted dying law until 2013, and no assisted deaths occurred under the law in that year, so the suicide rate cannot have been affected by an assisted dying law. Yet the picture is similar to Oregon's.
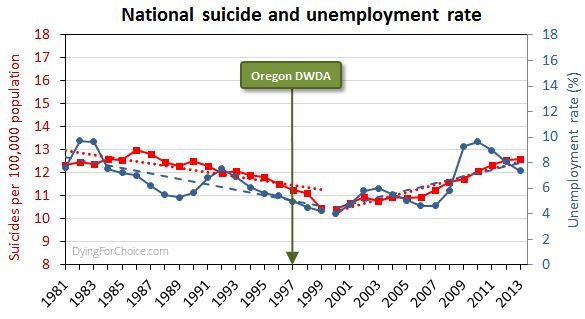
Here's the USA national suicide rate for the same period, with the unemployment rate added.
There are numerous and complex reasons for suicide and for changes in the rate, but a key one in this USA case is unemployment, which after falling in the 1990s rose abruptly from 2000 onwards.
Has Oregon's suicide rate been worsening relative to other USA states, though? The state annual suicide rankings are informative.
Prior to the DWDA, the trend in Oregon's suicide ranking among all USA states was deteriorating (where ranking number one is the highest suicide rate). Since the Act came into effect, the trend is improving. The difference in trends is statistically significant. In the sixteen years since the Act came into effect, Oregon has appeared in the "top ten" six times, compared with twelve times in the 16 years prior to the Act.
So, let's examine the three elements of the Catholic Church's statement:
1. "Since Oregon legislated, the standard suicide rate has increased remarkably and alarmingly"
This statement is false by omission. It is critically relevant to mention that Oregon's suicide rate dropped massively two years after the DWDA came into effect. Only after 2000 did it begin to rise—like most states and nationally—and in response to a rising unemployment rate.
2. "Oregon had a very, very low suicide rate prior to that [the DWDA]"
This statement is completely false. Oregon's mean rate suicide for 16 years after the act is not significantly different from the mean for 16 years prior to the Act. Indeed, government data back to 1968 shows Oregon's general suicide rate has always been high and never "low", let alone "very, very low".
3. It's not yet the largest rate in the US, but it's getting there"
This statement is completely false. Oregon's suicide ranking amongst USA states was worsening prior to the DWDA, but has been improving since.
It's very disappointing indeed that the Catholic Archdiocese of Melbourne would offer such profoundly false testimony to a legislative committee making inquiries on behalf of the people of Victoria. The offense is all the more grevious because of the unequivocal manner in which the statement was made, and that the witnesses specifically stated they did not bring any fanciful or frivolous arguments to the Committee.
It's time to comprehensively stamp out false information about assisted dying, no matter how fervently it might be believed by its proponents. Watch this space: there's plenty more to come!
Blog by Neil FrancisPosted on Sunday 22nd November 2015 at 5:05am
The Parliament of Victoria is conducting an inquiry into end-of-life decision making.
The standing Legal and Social Issues Comittee of the Parliament of Victoria, Australia, is currently conducting an inquiry into end-of-life decision making, to inform any legislative changes required in order to reflect contemprary views and best practice.
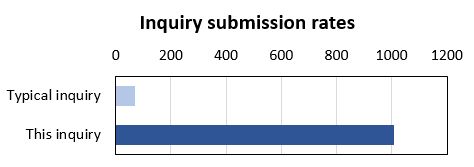
The inquiry has certainly engaged the community: it has received a record number of submissions. The Legal and Social Issues Committee typically receives a couple of dozen submissions to any of its inquiries, occasionally even sixty or eighty. In contrast, the inquiry on end-of-life decision making has received more than one thousand (1,017) submissions.
Most of the submissions (98%), including DyingForChoice.com's, are published on the Committee's website, with the tiny remainder kept confidential at the request of the submitter.
The terms of reference for the inquiry are completely silent on the matter of assisted dying. The Terms talk about "making informed decisions", "exercising preferences" and "the role of palliative care" in the context of current legislation and any required changes.
So, given that assisted dying is not mentioned in the Terms of Reference, you'd expect a modest number of submissions to address the issue, right? Wrong.
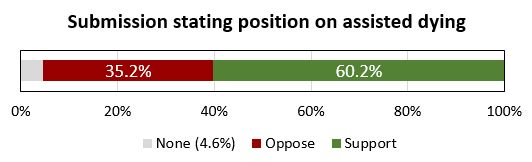
Of the submissions that are published on the Committee's website (and which I could therefore read), a staggering 95.4% of them make specific and deliberate points about assisted dying law reform, and 60.2% of the published submissions make points in favour of law reform to permit assisted dying in one form or another.
There is no clearer indication than this of how deeply engaged the Victorian public is with end-of-life decision making, and how important assisted dying law reform is to the options they might consider.
The Leglislative Council and this Committee are to be highly commended for establishing and conducting the inquiry. Public hearings with witness appearances have further helped inform the Committee and its Secretariat. The transcript of my appearance can be read here.
We the people of Victoria look forward with anticipation to the final report of the Committee, and the recommendations it makes. The Committee must report back to the Legislative Council no later than 31st May 2016. But, given the tsunami of submissions and the continuing public hearings, we won't be surprised if the Committee is granted an extension to complete its work.
Blog by Neil FrancisPosted on Sunday 15th November 2015 at 2:38am
ABC TV's Q&A panel discusses assisted dying law reform on 9th Nov 2015
In a recent opinion piece in the ABC’s Religion and Ethics section, Bernadette Tobin1 rails against assisted dying, commencing with the criticism that the ABC’s Q&A discussion on the subject this week “lacked precision.” But Tobin’s opinion piece itself commits exactly this offence, as I explain.
For the sake of brevity I’ll only quickly mention that Tobin’s piece also fails on the score of accuracy. For example, she wrongly asserts that “euthanasia” means a doctor administering lethal medication to a patient. It doesn’t. “Euthanasia” simply means “good death”: nothing more and nothing less, regardless of how it occurs. Tobin also asserts that voluntary euthanasia in lawful jurisdictions has caused non-voluntary euthanasia to develop. This is the polar opposite of published empirical research evidence.
But back to precision. Tobin employs two imprecise and deeply flawed arguments in her objection to assisted dying. She variously rolls them in together, so let’s unpack what they are: (A) the “it’s only fair” slippery slope, and (B) “it’s OK if you don’t mean it”.
A: The “It’s only fair” slippery slope
Tobin directly links assisted dying for the terminally ill to “anyone who is in pain, discomfort, constipated, incontinent, depressed, anxious and so on” by way of potential “benefit”. She conjectures that increasing the restrictions to who may qualify, and the process of qualification, would then be “unfair” to these others. She then goes on to extend the argument to those lacking in decisional capacity such as infants and those with Alzheimer’s. Surely, she says, “it would be ‘unfair’ to deny these people the ‘benefit’ that we will make available to those who are able to request it?”
Slippery slope indeed. And it’s wrong. Let me illustrate how, using a topic familiar in political debate over recent years: same-sex marriage.
Opponents of same-sex marriage law reform, when using arguments of the kind Tobin offers (as they often do), say that we can’t allow two men to marry, or two women to marry, because then we would have to allow three or more people to marry. Further down the slippery slope, we would have to allow people to marry animals. Don’t laugh: such things have been argued.
Next—given that under the Corporations Act 2001 (Cth), companies, owners’ corporations and incorporated associations are at law ‘persons’, and now that persons may marry—it would be “unfair” (note that I’ve used imprecision quotation marks around the word as Tobin does) to disallow people from marrying companies and companies from marrying each other.
Finally, using Tobin’s own line of argument, it would be “unfair” to deny infants and those with Alzheimer’s being married off for the alleged “benefit” (those quotation marks again) that everyone else is enjoying, so we must as an unavoidable consequence of the first step of allowing same-sex marriage, allow arranged marriages for babies and those with advanced dementia.
By now it’s easy to spot two terminal flaws in Tobin’s argument.
Firstly, the use of just one criterion (“fairness”—which she leaves imprecisely undefined) as the sole basis for decision making about this legislative reform is indefensible. What about other critical factors such as well-informed, rational, decisional capacity, judging and weighing what a “benefit” is, in the face of intolerable and unrelievable suffering, consistent with one’s own values and beliefs, who may decide, and the right not to participate?
Secondly, any slippery slope’s purported summit (from which changes are argued only to slip downwards) is deeply rooted in the normativity of the present. We are used to marriage being between a man and a woman. In our relative comfort we accept it as ‘normal,’ ‘good’ and the ‘right thing’.
In decision-making scholarship this normativity is known as “anchoring”. Like an anchor around which a boat will swing according to the wind and tide, we take the pivot point (the anchor of the now), as the natural starting point for future decisions, comparing changes only to the present state of affairs.
But it isn’t a valid anchor, and assuming that it is seriously biases our thinking. We need cast our anchor back just one mooring from the current point to see how the anchor tints our decision-making spectacles:
“We can’t allow a man and a woman to marry, because then it would be unfair to not allow two men to marry, or two women to marry, and then…”
Clearly, it is imperative that we outlaw marriage altogether.
The upshot of this slippery slope, when followed properly to its own logical conclusions, is that we must deny all rights because we can confect a slippery slope into a hypothetical moral abyss for any right.
B: It’s OK if you don’t mean it
Tobin further argues that relieving distressing symptoms “is good palliative care, even when that relief happens to hasten death.”
She doesn’t name it explicitly, but this is the doctrine of double effect, an argument first crafted in the thirteenth century by Catholic priest Thomas Aquinas. The doctrine suggests that a bad consequence of an action is justifiable if the agent did not intend the bad effect, if the intended good effect outweighs the bad effect, and if the agent applies diligence in attempting to minimise the bad effect. Notice that the doctrine speaks directly about the intentions of the agent and is silent on the views of the person upon whom the agent might act.
Tobin rails against a doctor intentionally administering a lethal dose to a patient (regardless of whether it is the dying patient’s most fervent wish) and slams the expressions “dying with dignity” and “aid in dying” as “fudges”.
Yet the doctrine of double effect, for which she argues in support, is itself a fudge because it says:
“It’s OK to for a doctor to decide to and actually kill their patient (after all, they hastened the patient’s death), as long as they don’t mean to, and they mean well.”
What kind of standard is the secret stuff that goes on inside a doctor’s head without reference of any kind to the patient’s own views and desires, when compared to a fully informed, documented and tested request from the patient?
It’s no wonder that many scholars (as do I) consider the doctrine of double effect problematic.
--
Bernadette Tobin is the Director of the Plunkett Centre for Ethics, a joint initiative of St Vincent’s Hospital, Sydney, and Australian Catholic University (ACU). According to ACU, a core mission of the Centre is to “bring a Catholic perspective to all its endeavours”.2
It’s unsurprising then that I detected neither broad thrust nor any detail of Tobin’s ABC opinion piece that deviated from the views of the Vatican. So be it.
There are many points on which Tobin and I agree, such as the potential benefits of palliative care for the dying. I argue, though, that basic scrutiny of the proffered 'principles' reveal them as deeply flawed and unpersuasive.
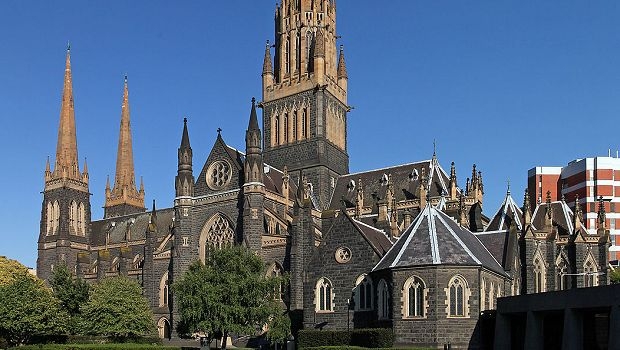
 Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Figure 1: The Belgium general suicide rate before and after assisted dying law reform