Blog by Neil FrancisPosted on Sunday 8th May 2016 at 9:48pm
Jeanne Smits' completely false statement in LifeSiteNews
Well it didn't take long. Recently I posted a fact-based report card on Dutch euthanasia practice, based on the actual data from the 2015 annual report (and all the earlier reports) of the Dutch Euthanasia Commission. Now, just a few days later, conservative religious opponents have begun publishing completely untrue statements about Dutch euthanasia practice.
Catholic blog LifeSiteNews' 'Paris correspondent' Jeanne Smits has bolted out of the misinformation blocks, assertively and categorically stating in respect of the small increase in number of euthanasia cases from 2014 to 2015, that:
"The rise is mainly due to the increase of euthanasia for demented, elderly people as well as psychiatric patients, two categories that raise even more questions than 'ordinary' euthanasia for untreatable physical pain."
Smits goes on to correctly report that dementia was an underlying factor in 109 of the cases in 2015 (against 81 in 2014) and psychiatric disorders in 56 patients (against 41 in 2014).
The total number of euthanasia cases increased from 5306 in 2014 to 5516 in 2015, an increase of 210 cases. The increase in dementia cases was 28 and in psychiatric disorders was 15. Therefore, underlying dementia accounted for 13% of the increase, and psychiatric disorders 7% of the increase.
Cherry-picking
Smits has cherry-picked just the dementia and psychiatric illness figures and presented them in a way that supports her story arc, painting a bleak picture.
But by no stretch of the imagination does dementia and psychiatric illness account "mainly" for the increase as she categorically states.
What didn't Smits report at all? Cancer: the Netherlands' leading cause of death. In 2015, cancer was the underlying condition in 4000 euthanasia cases, against 3888 in 2014, a rise of 112 cases or 53% of the increase. That compares with dementia at 13% and psychiatric illness at 7% (20% combined), which Smits selectively critiques as a 'sharp rise'.
In no way is Smits' statement true.
No, let's be frank: it's an outright lie. Cancer was the major underlying condition accounting for more than half of the small increase (4%) of cases in 2015.
More evidence refutes the claim
Comparing one years' data with just the preceding years' data can be misleading when the number of observations is low, as it is for dementia and psychiatric illness euthanasia cases. Fortunately, we have data for more than just the one year.
Since 2012 the Euthanasia Commission has consistently published specific figures for dementia and psychiatric illness cases, so we can compare a rise over four years rather than just one. On this basis as a proportion of total 2012 cases, there has been a 17.9% increase in cancer-related cases, a 1.6% increase in dementia cases, and a 1.0% increase in psychiatric illness cases.
Longitudinal data is even more clear than a single year. It unequivocally refutes Smits' silly claim.
Bull is spread
Does Smits' claim matter much? Won't it just slip into oblivion?
No. Michael Haverluck of the conservative Christian paper OneNewsNow has already picked up Smits' article and repeated her claim as gospel. It remains to be seen how many other anti-euthanasia bloggers republish this nonsense.
Unacceptable conduct
In my view, publishing such a categorical yet false statement — even when unintentional — without first properly checking the facts, is unacceptable conduct. The article (and its derivatives) ought to be withdrawn.
Blog by Neil FrancisPosted on Wednesday 25th November 2015 at 8:00pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
On Wednesday 19th November 2015, the Catholic Church appeared before the Victorian Parliament's Legal and Social Issues Committee. Monsignor Anthony Ireland, the Episcopal Vicar for Health, Aged and Disability Care, and Father Anthony Kerin, Episcopal Vicar for Life, Marriage and Family gave evidence about end-of-life decision making. They made a factually wrong allegation about Oregon during their testimony.
Anthony Ireland spoke first, making it clear that they were appearing before the Committee with delegated authority from the Catholic Archbishop of Melbourne (Denis Hart) and with the endorsement of the Victorian Catholic Bishops. He emphasised that "the Catholic Archdiocese of Melbourne does not come to this Committee with fanciful or frivolous arguments."
During question time. Committee Chair Edward O'Donohue asked the Vicars if they had any evidence from lawful jurisdictions to back up their claim that legalising assisted dying would result in a significant reduction in medical research. The Vicars flailed about with vague hypotheticals, but no evidence.
Committee Deputy Chair Nina Springle remarked that some of their testimony was inconsistent with direct evidence from lawful jurisdictions and invited them to reflect on the contradictions. To this, Anthony Kerin stated:
"We know, for example, since Oregon legislated, that the standard suicide rate has increased remarkably and alarmingly. It's not yet the largest rate in the US, but it's getting there, when Oregon had a very, very low suicide rate prior to that."
Let's not mince words: the allegation is comprehensively false. In fact it's three false statements all wrapped up into one.
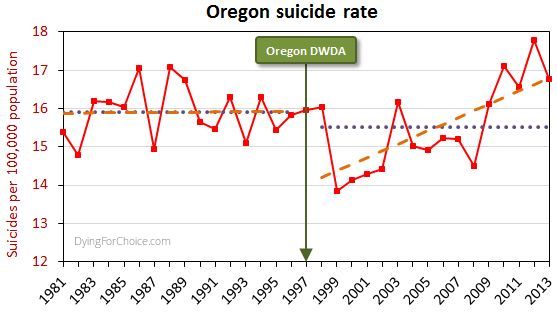
The USA government's CDC mortaility database provides solid empirical data. Here's Oregon's longitudinal suicide rate statistics, including sixteen years before its Death With Dignity Act (DWDA), and sixteen years after.
Here are the pertinent facts about Oregon's general suicide rate:
The average for the 16 years after the DWDA is lower than, but not statistically different from, the 16 years prior to the Act.
There was a massive drop in the suicide rate two years after the DWDA came into effect, and the rate has risen only from there.
The rise from 2000 onwards is repeated in the majority of USA states and in the national average. The trend increase in Oregon is not statistically different from the national trend increase.
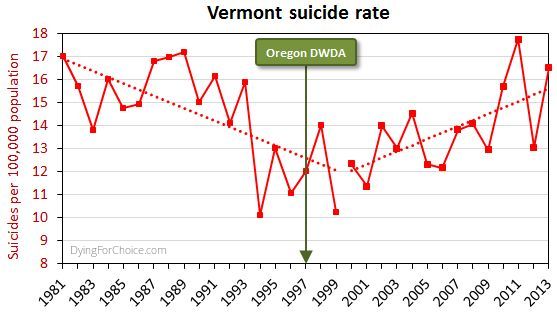
By way of comparison, here's Vermont's suicide rate for the same period.
Now, Vermont didn't have an assisted dying law until 2013, and no assisted deaths occurred under the law in that year, so the suicide rate cannot have been affected by an assisted dying law. Yet the picture is similar to Oregon's.
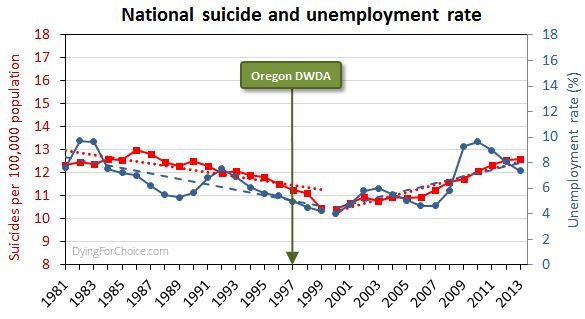
Here's the USA national suicide rate for the same period, with the unemployment rate added.
There are numerous and complex reasons for suicide and for changes in the rate, but a key one in this USA case is unemployment, which after falling in the 1990s rose abruptly from 2000 onwards.
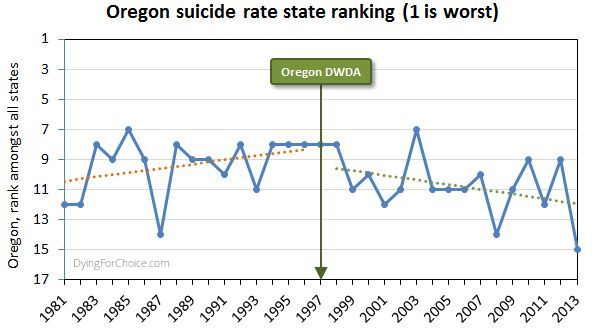
Has Oregon's suicide rate been worsening relative to other USA states, though? The state annual suicide rankings are informative.
Prior to the DWDA, the trend in Oregon's suicide ranking among all USA states was deteriorating (where ranking number one is the highest suicide rate). Since the Act came into effect, the trend is improving. The difference in trends is statistically significant. In the sixteen years since the Act came into effect, Oregon has appeared in the "top ten" six times, compared with twelve times in the 16 years prior to the Act.
So, let's examine the three elements of the Catholic Church's statement:
1. "Since Oregon legislated, the standard suicide rate has increased remarkably and alarmingly"
This statement is false by omission. It is critically relevant to mention that Oregon's suicide rate dropped massively two years after the DWDA came into effect. Only after 2000 did it begin to rise—like most states and nationally—and in response to a rising unemployment rate.
2. "Oregon had a very, very low suicide rate prior to that [the DWDA]"
This statement is completely false. Oregon's mean rate suicide for 16 years after the act is not significantly different from the mean for 16 years prior to the Act. Indeed, government data back to 1968 shows Oregon's general suicide rate has always been high and never "low", let alone "very, very low".
3. It's not yet the largest rate in the US, but it's getting there"
This statement is completely false. Oregon's suicide ranking amongst USA states was worsening prior to the DWDA, but has been improving since.
It's very disappointing indeed that the Catholic Archdiocese of Melbourne would offer such profoundly false testimony to a legislative committee making inquiries on behalf of the people of Victoria. The offense is all the more grevious because of the unequivocal manner in which the statement was made, and that the witnesses specifically stated they did not bring any fanciful or frivolous arguments to the Committee.
It's time to comprehensively stamp out false information about assisted dying, no matter how fervently it might be believed by its proponents. Watch this space: there's plenty more to come!
Blog by Neil FrancisPosted on Sunday 15th November 2015 at 2:38am
ABC TV's Q&A panel discusses assisted dying law reform on 9th Nov 2015
In a recent opinion piece in the ABC’s Religion and Ethics section, Bernadette Tobin1 rails against assisted dying, commencing with the criticism that the ABC’s Q&A discussion on the subject this week “lacked precision.” But Tobin’s opinion piece itself commits exactly this offence, as I explain.
For the sake of brevity I’ll only quickly mention that Tobin’s piece also fails on the score of accuracy. For example, she wrongly asserts that “euthanasia” means a doctor administering lethal medication to a patient. It doesn’t. “Euthanasia” simply means “good death”: nothing more and nothing less, regardless of how it occurs. Tobin also asserts that voluntary euthanasia in lawful jurisdictions has caused non-voluntary euthanasia to develop. This is the polar opposite of published empirical research evidence.
But back to precision. Tobin employs two imprecise and deeply flawed arguments in her objection to assisted dying. She variously rolls them in together, so let’s unpack what they are: (A) the “it’s only fair” slippery slope, and (B) “it’s OK if you don’t mean it”.
A: The “It’s only fair” slippery slope
Tobin directly links assisted dying for the terminally ill to “anyone who is in pain, discomfort, constipated, incontinent, depressed, anxious and so on” by way of potential “benefit”. She conjectures that increasing the restrictions to who may qualify, and the process of qualification, would then be “unfair” to these others. She then goes on to extend the argument to those lacking in decisional capacity such as infants and those with Alzheimer’s. Surely, she says, “it would be ‘unfair’ to deny these people the ‘benefit’ that we will make available to those who are able to request it?”
Slippery slope indeed. And it’s wrong. Let me illustrate how, using a topic familiar in political debate over recent years: same-sex marriage.
Opponents of same-sex marriage law reform, when using arguments of the kind Tobin offers (as they often do), say that we can’t allow two men to marry, or two women to marry, because then we would have to allow three or more people to marry. Further down the slippery slope, we would have to allow people to marry animals. Don’t laugh: such things have been argued.
Next—given that under the Corporations Act 2001 (Cth), companies, owners’ corporations and incorporated associations are at law ‘persons’, and now that persons may marry—it would be “unfair” (note that I’ve used imprecision quotation marks around the word as Tobin does) to disallow people from marrying companies and companies from marrying each other.
Finally, using Tobin’s own line of argument, it would be “unfair” to deny infants and those with Alzheimer’s being married off for the alleged “benefit” (those quotation marks again) that everyone else is enjoying, so we must as an unavoidable consequence of the first step of allowing same-sex marriage, allow arranged marriages for babies and those with advanced dementia.
By now it’s easy to spot two terminal flaws in Tobin’s argument.
Firstly, the use of just one criterion (“fairness”—which she leaves imprecisely undefined) as the sole basis for decision making about this legislative reform is indefensible. What about other critical factors such as well-informed, rational, decisional capacity, judging and weighing what a “benefit” is, in the face of intolerable and unrelievable suffering, consistent with one’s own values and beliefs, who may decide, and the right not to participate?
Secondly, any slippery slope’s purported summit (from which changes are argued only to slip downwards) is deeply rooted in the normativity of the present. We are used to marriage being between a man and a woman. In our relative comfort we accept it as ‘normal,’ ‘good’ and the ‘right thing’.
In decision-making scholarship this normativity is known as “anchoring”. Like an anchor around which a boat will swing according to the wind and tide, we take the pivot point (the anchor of the now), as the natural starting point for future decisions, comparing changes only to the present state of affairs.
But it isn’t a valid anchor, and assuming that it is seriously biases our thinking. We need cast our anchor back just one mooring from the current point to see how the anchor tints our decision-making spectacles:
“We can’t allow a man and a woman to marry, because then it would be unfair to not allow two men to marry, or two women to marry, and then…”
Clearly, it is imperative that we outlaw marriage altogether.
The upshot of this slippery slope, when followed properly to its own logical conclusions, is that we must deny all rights because we can confect a slippery slope into a hypothetical moral abyss for any right.
B: It’s OK if you don’t mean it
Tobin further argues that relieving distressing symptoms “is good palliative care, even when that relief happens to hasten death.”
She doesn’t name it explicitly, but this is the doctrine of double effect, an argument first crafted in the thirteenth century by Catholic priest Thomas Aquinas. The doctrine suggests that a bad consequence of an action is justifiable if the agent did not intend the bad effect, if the intended good effect outweighs the bad effect, and if the agent applies diligence in attempting to minimise the bad effect. Notice that the doctrine speaks directly about the intentions of the agent and is silent on the views of the person upon whom the agent might act.
Tobin rails against a doctor intentionally administering a lethal dose to a patient (regardless of whether it is the dying patient’s most fervent wish) and slams the expressions “dying with dignity” and “aid in dying” as “fudges”.
Yet the doctrine of double effect, for which she argues in support, is itself a fudge because it says:
“It’s OK to for a doctor to decide to and actually kill their patient (after all, they hastened the patient’s death), as long as they don’t mean to, and they mean well.”
What kind of standard is the secret stuff that goes on inside a doctor’s head without reference of any kind to the patient’s own views and desires, when compared to a fully informed, documented and tested request from the patient?
It’s no wonder that many scholars (as do I) consider the doctrine of double effect problematic.
--
Bernadette Tobin is the Director of the Plunkett Centre for Ethics, a joint initiative of St Vincent’s Hospital, Sydney, and Australian Catholic University (ACU). According to ACU, a core mission of the Centre is to “bring a Catholic perspective to all its endeavours”.2
It’s unsurprising then that I detected neither broad thrust nor any detail of Tobin’s ABC opinion piece that deviated from the views of the Vatican. So be it.
There are many points on which Tobin and I agree, such as the potential benefits of palliative care for the dying. I argue, though, that basic scrutiny of the proffered 'principles' reveal them as deeply flawed and unpersuasive.
News reportPosted on Monday 5th October 2015 at 4:15pm
On Friday September 11th 2015, the California legislature passed an assisted dying bill, the End Of Life Option Act, modelled on the Oregon Death With Dignity Act which has been in effect since 1997. It had been a long and tortuous wait to see if Governor Jerry Brown would sign the Bill into law.
It is reported that Governor Brown struggled to decide whether to sign the Bill which was actively opposed by the Catholic Church. Governor Brown is a former Jesuit seminary student. He sought views from his doctors, from a Catholic Bishop, from disability advocates, retired South African Archbishop Desmond Tutu and others, to reach a decision. While he had given no indication of his views or intention to sign, historically he has supported abortion rights, contrary to the teachings of the Vatican.
On Monday October 5th, he signed the Bill. It will come into effect 90 days after the California legislature adjourns its special session on healthcare. But that may not be for some months yet, even as long as late next year.
Governor Brown said "I have considered the theological and religious perspectives that any deliberate shortening of one's life is sinful."
"I do not know what I would do if I were dying in prolonged and excrutiating pain. I am certain, however, that it would be a comfort to be able to consider the otpions afforded by this bill. And I wouldn't deny that right to others," he wrote in his affirmation of the Bill.
California joins Oregon, Washington, Montana and Vermont to afford their citizens the respect to make their own decicions about the possibility of a hastened death at the end of life. Around one in six Americans now has legal access to restricted assisted dying.
Dissatisfied that the legislature and the Governor have spoken on behalf of the overwhelming majority of Californians who support the measure, Catholic-backed Californians Against Assisted Suicide is considering a range of countermeasures, including a legal challenge and a referendum.
Blog by Neil FrancisPosted on Tuesday 8th September 2015 at 5:16am
It was inevitable, the latest attempt by senior British clergy to persuade politicians to reject Lord Joffe’s Assisted Dying for the Terminally Ill Bill. Led by the Archbishop of Canterbury, Justin Welby—whose predecessor Lord Carey now supports the reform—nine clergy sent a letter to ‘remind’ Parliament of supposed terrible consequences.
So what points did the clerics offer to Parliamentarians, and are they valid? Let’s take a look at each of the five ‘reasons’ advanced in order to deny Brits assisted dying choice.
Firstly, the clerics argue that the ‘answer’ is palliative care. Britain boasts the world’s gold standard in palliative care practice and it’s a great credit to practitioners. But the medical literature as well as the experience of the dying and their loved ones is conclusive: palliative care simply can’t always help. Experts say that “relief of suffering remains an elusive goal for many patients” and it’s “clear that improving palliative care will not remove the need for legalizing assisted dying.”
The premise of palliative care is to provide interventions. However, sometimes, not only does interventionism fail to help, it can itself be a source of suffering. And the individual may not want interventions, but rather to alight from the train of terminal illness one or two stops before the inevitable and intolerable terminus.
Secondly, the clerics argue that jurisdictions with assisted dying laws are facing serious problems, including wrongly claiming that the Dutch are now campaigning to include dementia as a basis to seek an assisted death. This right has been enshrined in Dutch law through advance care directives since 2002. In practice, the request is largely declined by doctors.
The clerics complain that dying patients in assisted dying jurisdictions are now using the law—hardly a surprising outcome given the proportion of people now dying of cancer in their later years.
They complain about supposed ‘doctor shopping’ in Oregon. If the patient’s first (or second) doctor declines a request to consider an assisted death on the basis of the doctor’s own convictions, are these clerics suggesting that the patient ought to have their right to lawful assessment denied, because their first doctor or two were religiously opposed?
Thirdly, the clerics argue that the majority of doctors are opposed to assisted dying law reform, ironically pointing out that a quarter to a third of doctors support reform. Why should Brits be denied a choice because two thirds of doctors currently won’t participate in that choice? (What proportion of doctors would participate in abortions, currently legal?) And doctors—who make up fewer than one in two hundred Brits—don’t elect Parliament, so why are their diverse views a case for outright denial?
Let’s name this argument for what it is: an appeal to apparent ‘authority’. Clerical ‘authorities’ (who don’t represent their flocks who are overwhelmingly in favour of reform) are making an appeal of medical ‘authorities’ as the reason to reject something the public believes should be a right. Paternalism indeed.
The fourth argument spreads an icing of hubris on the cake of objections. The clerics argue that the public really don’t understand and don’t know what they mean when the great majority keep saying ‘yes’ to repeated polls on assisted dying law reform.
Public opinion in fact demonstrates the opposite of gullibility: rejection of the attempted scare campaigns of religious ‘authorities’.
Fifthly (and thankfully lastly), the clerics argue that a right to choose assisted dying will inevitably become a duty to choose it. If the theory that ‘a right becomes a duty’ were an argument to reject one right, then all rights would necessarily be rejected on precisely the same principle.
Enshrined in the Mental Capacity Act 2005, Brits already have a right to refuse any medical treatment, even if life-saving. A Jehovah’s Witness may refuse a simple blood transfusion. An elderly person may refuse burdensome surgery. Yet the right to refuse treatment can theoretically become a duty to refuse, in exactly the same manner.
If the clerics genuinely believe their theory then they would argue to Parliament with equal force that the right to refuse medical treatment should be rescinded. Why don’t they?
The real reason for opposing the assisted dying Bill appears in the letter’s preamble: the clerics “hold all human life sacred”, in other words, a ‘gift from God’. Yet contemporary British Social Attitudes surveys reveal that the majority of Brits are not religious.
So the real question for the Parliament is this: should indefensible arguments put forward by a few clerical ‘authorities’ form a basis for denying choice wanted by the overwhelming majority of voters?
Blog by Neil FrancisPosted on Thursday 23rd July 2015 at 1:22am
The Victorian Premier doesn't support assisted dying law reform - at this stage.
Victorian Premier Daniel Andrews reports that he doesn’t support voluntary euthanasia “at this stage” (The Age, 21 Jun 2015), and that his objections are not based on his Catholic faith. I think it is fair to take him at his word given his historical record in facilitating conversation and reform around values-based issues such as abortion. But his current thinking on assisted dying is indefensible as I explain.
We know from repeated Newspoll Australia studies that amongst the millions of Victorians who want the State to respect their wish to make their own choices at the end of life, three out of four Australian Catholics are in favour of legalised assisted dying—at odds with the ‘traditional’ Catholic stance. Mr Andrews, like a majority of Catholic Australians, may simply not agree with the Vatican line on assisted dying choice, as they don't on a range of matters.
Mr Andrews says that his current objections instead revolve around ‘safeguard’ and ‘balance’ issues in a context of finite healthcare resources.
The Medical Treatment Act 1988 confers the right to Victorian patients to refuse any medical treatment. The right applies even if the treatment is life-saving, for example a simple blood transfusion. The Act contains no ‘safeguards’, as the Premier refers to them:
The patient is not required to give any reason;
The doctor is not required to inform the patient of their condition or likely consequences of any treatment or its refusal;
The doctor is not required to consider or assess the patient’s mental capacity to decide including depression;
The doctor is not required to recommend a palliative consult (if relevant);
The doctor is not required to consult any colleagues for a further opinion about the patient’s illness or mental capacity;
There is no obligation on the patient to consider their decision again after a short time;
While there is a standard form 'Refusal of Medical Treatment' document that can be signed to provide documentary evidence of the refusal, it is not mandatory;
There is no mandated path of reporting or review.
Indeed, a doctor who goes on to administer medical interventions to the patient who has refused them is guilty of the offence of ‘medical trespass’ and can be prosecuted.
Further, it is quite legal for a patient to decide to die by voluntary refusal of food and fluids, an option suggested as appropriate by Dr Bill Sylvester in an IQ2 debate at Melbourne Town Hall in November 2012, to a hostile reaction from the audience. Some doctors provide respite care to patients choosing this path. however, like refusal of medical treatment, there are no legislated safeguards.
On the basis of these two kinds of end-of-life decision making that have been lawful for at least a quarter century in Victoria, and which have no legislated safeguards, what evidence do we have of the so-called ‘slippery slope’ of resource-strapped healthcare providers or greedy relatives persuading the sick to choose a path to die earlier rather than later?
Both Victoria Police and the former Minister for Health, the Hon. David Davis, have advised that there are no known prosecutions under the provisions of the Medical Treatment Act 1988 for such inappropriate persuasion.
So, in Victoria we have the experience of two forms of decision-making whose direct and foreseeable consequence is death, with no mandated safeguards and within 'finite healthcare resources' (which Mr Andrews refers to as his reason), not resulting in prosecutions for persuasion to 'choose' death.
If Mr Andrews’ argument is that terminally ill Victorians ought to be denied the right to choose assisted dying because of supposed slippery slopes of persuasion, that argument would exactly and equally apply to the refusal of life-saving medical treatment and to the refusal of food and fluids.
Surely his Government is not suggesting that the existing rights be rescinded: that patients be forced to receive any and all life-saving and life-prolonging treatment in order to avoid a 'persuasion' bogeyman who doesn’t exist?
The Premier's stance is even less defensible in the light of proposed assisted dying legislation which includes a suite of checks and balances that are absent from existing rights.
Some dying individuals, reflecting upon their circumstances and deeply-held values and beliefs, determine that alighting from the train of terminal illness one or two stops before the terminus is a vastly better option than being forced to endure the train ride until the very end. We compound their indignities by saying it’s OK to decide to starve yourself to death (and we might even provide support along the way), but not OK to decide to die peacefully surrounded by loved ones at a predetermined time.
It is commendable that the Legislative Council has resolved to investigate the issue of end-of-life decisions, and whose final report will better inform the Premier and all Parliamentarians. Submissions to the Committee are open until Monday 31st August.
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:28pm
The opinion piece in The Age.
In today’s Fairfax press, Sydney woman Mary Ticinovic advances a number of reasons as to why she believes that assisted dying is not merciful. The by-line identifies her as a “clinical psychologist”. But her arguments are not founded on the basic tenets of psychology. How so?
Mary argues that to support assisted dying is to go “against the principle that all life is precious.” She offers no substantive explanation, invoking the notion of ‘human worth’, stating that it exists regardless of the health state or suffering of the person, and complaining that assisted dying promotes the idea that “your life is no longer worth living”.
These are not psychological arguments. We can agree that life is precious. But reluctantly deciding to hasten one’s death in the face of intolerable and unrelievable terminal suffering doesn’t negate that preciousness. Indeed, to some people, choosing assisted dying can evidence the preciousness of one’s very capacities and values as a human.
Whose standards?
Mary further muses over “by whose standards would we judge if life is not worthwhile any more”, as though this is only some vague theoretical argument amongst philosophers or doctors. This is not a psychological argument, either. Under assisted dying law reform, it is only the dying individual’s world-view and circumstances that determine whether he or she feels life is worth living: not anyone else. General philosophical theory doesn’t come into it.
She further argues that assisted dying “promotes a utilitarian view of humanity”. This is not a psychological argument, either. Nor is it valid. Indeed, legalised assisted dying respects the very nature of the diversity of humanity by enabling the world-views many people hold most dear: that of making rational choices consistent with their own beliefs, values and circumstances. Some patients, for example in Oregon, are deeply religious and believe that their God is compassionate and understands and respects their choice to avoid intolerable suffering. That’s not utilitarian at all.
Harm and the Hippocratic Oath
Mary invokes the Hippocratic Oath said by her medical friends to oblige doctors to “do no harm” and that the medical role is “in healing and helping the patient to be restored to health.” This is simplistic nonsense, not a psychological argument.
Firstly, doctors do harm all the time: think of surgical procedures or chemotherapy. Many medical interventions do harm, but we accept the harm because we expect there to be a commensurately greater good as a result.
Secondly, medical practice cannot always “restore the patient to health” as Mary exclusively puts it. What then? The dying patient may judge that the unrelievable suffering they will experience along the path to death is a greater harm than dying a little earlier. And, doctors also have a primary duty to relieve suffering, which Mary doesn’t mention. What is under review is whether a doctor may participate in the relief of intolerable and unrelievable suffering— by hastening death—if the patient believes this is the lesser harm.
Thirdly, the Hippocratic Oath is around 2,300 years old. It requires doctors to swear allegiance to ancient Greek gods. It forbids women from becoming doctors. It requires current doctors to train the next generation free of charge, and it forbids surgery. Contemporary doctors don’t take it, and it’s certainly not “part of training” as Mary mistakenly states.
None of these are psychology arguments.
'Sucker’s choice'
Mary then argues that requiring dying patients to endure until the end promotes—and that assisted dying prevents—“fostering gratitude”, “reconciling hurts or differences with family members or friends” and “showing them strategies or different ways to approach their pain and suffering”.
But, in jurisdictions where assisted dying is legal, for example in Oregon in the USA, these are precisely things that are encouraged under assisted dying. Doctors are required to inform applicants of available medical and palliative interventions. Family gathers on notice of an anticipated death, music and poetry is shared, and expressions of love, devotion and gratitude are exchanged.
If a dying patient has no intention of reconciling with family or reflecting on approaches to dealing with their pain and suffering under an assisted dying law, precisely the same intention applies to the current regime that requires the patient to endure until the end. To assume a difference is a false dichotomy.
Obligatory compassion
Mary also argues that assisted dying ought to remain outlawed because “nursing a sick loved one is a way to give back”. This is yet another specious non-psychology argument. It promotes the ‘right’ of the ‘nurse’ to express love and devotion through ‘caring interventions’ at the expense of the dying patient’s own world view and deeply-held wish for a hastened death. Now who’s being utilitarian?
The upshot
I ran Mary’s opinion piece past an experienced psychologist, who described it as little to do with psychology. Note that neither of us has experience of or is commenting on Mary’s expertise as a clinical psychologist: she may indeed be a very good one.
My associate wondered out loud if Mary’s arguments were based more on underlying religious views than anything else. I agreed: they seemed to me remarkably consistent with the arguments advanced by religious opponents, even though they avoided directly religious words. So I did a little research.
It turns out that Mary is a committed and active Sydney Catholic.* Evidence abounds of her devotion to the Catholic tradition, and I commend her for her conscientious reflective practice and participation in it.
However, I argue that neither the stated psychological qualification nor the unstated religious affiliation make the offered arguments valid.
-----
* By way of fairness, I place on the record that I am agnostic.