Blog by Neil FrancisPosted on Thursday 23rd May 2019 at 2:39am
Palliative care specialist advances incoherent reasons to oppose VAD.
Director of Palliative Care at Cabrini Health, Associate Professor Natasha Michael, yesterday published an opinion piece in The Age newspaper. In it, she rails against Victoria’s voluntary assisted dying (VAD) Act which comes into effect on 19th June. Instead she articulates an arrogant and prescriptive view of what Australians should and shouldn’t be allowed, consistent with Catholic dogma, as I uncover.
Michael, along with fellow devout Catholic Dr Stephen Parnis, ‘tirelessly’ opposed the introduction of Victoria’s VAD law. They continue to actively oppose it, and her opinion piece reveals her spurious ‘reasoning’.
The Catholic Healthcare brick wall
More than half of all palliative care services in Australia are delivered through Catholic institutions, of which Cabrini Health is one arm. These institutions have determined that VAD will not be available in any of their facilities or via any of their services, even if the individual patient and doctor are supportive.
This arbitrarily limits access to lawful choice by citizens.
Confected ‘institutional conscience’
I say ‘arbitrarily’ because ‘institutional conscience’ is a confection: it doesn’t really exist. Only real persons have conscience. The fabricated dictates of any institution — presented as ‘moral rules’ — extinguish the actual real conscience of those who exist within it: at least, those whose conscience differs.
The upshot is that a specific cohort of religious, celibate men in Rome dictate whether Australian citizens can or can’t obtain lawful healthcare services from half the service providers.
So let’s examine what the institutional ‘conscience’ has to say.
Disgraceful framing in headline
“We can’t let voluntary assisted dying negate our commitment to the ill”, Michael’s article headline screams.
Firstly, VAD is not available to the “ill”. It’s available only to those with terminal illness and intolerable suffering, according to 68 criteria.
Secondly, Michael invokes a false dichotomy of “negating a commitment”. VAD does not “negate a commitment”. Indeed, to fail to hear and respect a persistent, fully informed and tested request for VAD that meets all the criteria is to negate palliative care’s commitment to honour the patient’s deeply held values, beliefs and decisions.
Medical-coloured glasses
“The introduction of voluntary assisted dying legislation in Victoria on June 19 will remind us of the occasional failure of medicine,” Michael says.
That’s it. The patient’s death is a failure of medicine, as though a person’s death is a medical event rather than a deeply human and private one of personhood.
It also flags the common but immature medical assumption that “death = failure”. Death is inevitable, not a “failure”. The key question about death for people with terminal illness is “how”, and Michael presumes to prescribe the “how”: being receptacles for interventions that she and her colleagues provide.
Let’s be clear. Many people are helped enormously by palliative care. That’s a great credit to the discipline’s specialists.
However, as Palliative Care Australia acknowledges, even the best palliative care can’t relieve all excruciating, debilitating and humiliating refractory symptoms.
Michael’s answer to this sometimes “failure” of medical interventions? Deliver more interventions, whether the patient considers them consistent with his own values, beliefs and circumstances or not.
They’re very heavily medical-coloured glasses indeed.
Three faux ‘threats’
Michael then invokes three faux ‘threats’ supposedly caused by lawful VAD in Victoria.
Faux threat 1: “Validating suicide as an acceptable choice”.
Michael exposes her own bias here: that all self-hastening of deaths are the same — that there is no meaningful difference between a dying person who is fully informed and whose rational choice for a peaceful assisted death has been extensively tested, with the violent and impulsive action of a person suffering a temporary, resolvable personal crisis, be it mental illness, substance abuse, intimate relationship breakdown or other circumstance.
Michael is pretty much on her own here. Most Australian doctors make a clear distinction between these very different contexts.
Faux threat 2: “accepting substandard medical care by supporting the lack of rigour in defining [VAD] eligibility”.
Michael overlooks that there is a major lack of rigour in existing, lawful end-of-life choices.
There are no statutory requirements for a patient to refuse medical treatment, even if the treatment would be life-saving.
There are no statutory requirements for the voluntary refusal of food and fluids in order to die, either.
More critically, despite terminal sedation being a common end-of-life medical practice but ethically problematic (including that it may hasten death and may not alleviate intractable symptoms), not only is there no statutory requirement for its practice, but neither the Australian Medical Association nor Palliative Care Australia have official guidelines on its practice.
Thus, in railing against the staggering 68 standards of practice prescribed in Victoria’s VAD law — vastly more than any other in the world — as a “lack of rigour”, Michael makes no mention of three other major life-end choices that have no such standards, including her own discipline’s terminal sedation.
Doctor, heal thyself (and thine own systems).
Faux threat 3: “introducing into the healthcare curriculum the intentional ending of life as acceptable medical treatment”
Michael creates a misleading impression here. By referring to ‘curriculum’ you might think that all medical students would have to undergo training on how to end lives, or be ‘indoctrinated’ to accept VAD. That is not true.
To be able to prescribe lethal medication under Victoria’s legislation, the doctor must undergo additional training in relation to that procedure. Doctors will only receive the training if they self-nominate for it: it’s not compulsory.
If, by ‘curriculum’ Michael means only “VAD might be discussed” in medical school, then she would have to articulate why termination of pregnancy (to which the Catholic church objects) should not be discussed, either. Nor the transfusion of blood, since many Jehovah’s Witnesses object to the procedure.
Own failure in palliative care principles
Nowhere in her opinion piece does Michael acknowledge that the patient may deeply hold values and beliefs that validly favour VAD. Thus, Michael offends the first principle of palliative care which is to make the patient the centre of care and to honour as much as possible the patient’s values, beliefs, attitudes and wishes.
Indeed, in her conclusion, Michael states that palliative care “remains committed to the ongoing accompaniment of our patients. Not abandoning them” and which is “the only plausible method of compassion and care.”
This surely is the most egregious and arrogant self-interest of all: patients must subject themselves to being accompanied by palliative care staff and their ‘interventions’ whether they want more or not.
On the contrary, to fail to hear and respect a genuine, informed and persistent request for a peaceful hastened death from a dying patient for whom this accords most firmly with his deeply held values and beliefs, is to abandon the patient.
Conclusion
Michael is of course entitled to her personal stance, and I celebrate her right to hold her views: for herself.
However, her ‘requirement’ that all Victorians be denied access to an option that four out of five believe to be moral — and instead subject themselves to interventions administered by Michael and her colleagues — reveals an unattractive arrogance.
It’s a shame that Catholic bioethics doesn’t teach more about reflection, especially as to whether one’s own beliefs ought to dictate and limit the choices of others with equally firmly held, though different, values.
In the meantime, Victorians are pawns to the tyranny of the Vatican as to whether there is a local healthcare facility that will hear and examine their request for a peaceful, assisted death in the face of terminal illness.
Blog by Neil FrancisPosted on Thursday 12th October 2017 at 1:50am
The latest religious right 'think tank' lobby group, the Institute for Civil Society.
I challenge the latest religious right commentators opposing Victoria’s Voluntary Assisted Dying Bill to skip the flip-flopping and engage constructively.
They’re at it again. This time it’s the religious right’s latest ‘think tank’ front group, the impressively-named Institute for Civil Society. Sounds grand, doesn’t it?
But if you look into their lot in life, it’s to protect ‘religious freedoms.’ By that, they mean the right to lawfully discriminate against others of whom they disapprove, while at the same time arguing that they not be discriminated against.
Mark Sneddon and Sharon Rodrick of the ‘Institute’ published an opinion piece in Fairfax Media today.
In it, they slam the Victorian Government’s Voluntary Assisted Dying Bill, which was introduced into the Parliament recently.
They level several criticisms at the Bill to say it's not 'safe'. But they could have advanced any criticism of the Bill to claim, as they do, that “the vulnerable will be at risk” — a logical fallacy as I’ve pointed out before. The "vulnerable will be at risk", by circular definition, if the Bill is printed in black ink (as it is) instead of purple, but they didn't complain about the colour of the ink.
The flip-flop
The point is, they flip-flop because they’re remarkably inconsistent in their position. At the same time as pointing out supposed flaws in the Voluntary Assisted Dying Bill, demanding a much higher standard of proof about a number of things, they completely fail in their opinion piece to even mention — let alone demand the same level of safeguards for — an already-legal and equivalent hypothetical risk for the “vulnerable.”
Equivalent hypothetical risk in operation for nearly 30 years
In Victoria, patients have an inalienable right to refuse any and all medical treatment. No reason need be given, even if the treatment is life-saving. The Medical Treatment Act 1998, currently in force, has several safeguards to protect against coercion or undue influence. In Section 5(1), one doctor and “another person” (who can be anybody) must be satisfied that:
“the patient has clearly expressed or indicated a decision”; and
“the patient’s decision is made voluntarily and without inducement or compulsion”; and
“the patient has been informed” about their condition and “has appeared to understand that information”; and
“the patient is of sound mind and has attained the age of 18 years.”
They’re all the legislated safeguards for the refusal of life-saving medical treatment.
And how many cases of undue influence have been prosecuted in Victoria over the nearly 30 years the Medical Treatment Act 1998 has been in effect? Precisely none. Not one.
So much for Messrs Sneddon and Rodrick’s avaricious relatives lurking at every bedside.
A new, equivalent hypothetical risk
The Medical Treatment Planning and Decisions Act 2016, which will come into force in March next year and which extinguishes the Medical Treatment Act 1998 at that time, also contains several similar safeguards for the refusal of life-saving medical treatment.
In witnessing an Advance Care Directive (Section 17), the two signatories, only one of whom must be a medical doctor, must certify that:
the person “appeared to have decision-making capacity” in relation to the documented decisions; and
the person “appeared to understand the nature and effect of each statement”; and
“the person appeared to freely and voluntarily sign the document”; and
“the person signed the document in the presence of the two witnesses”; and
“the witness is not an appointed medical treatment decision maker for the person.”*
In Section 52 of the Act, a health practitioner is forbidden to administer medical treatment if they are aware the patient has refused it, however (lawfully) refused.
This Act was passed in the term of the current Parliament: that is, by the same State MPs who are now considering the Voluntary Assisted Dying Bill.
There was no great fracas over the sensible safeguards spelled out in the new Medical Treatment Planning and Decisions Act. There was no onslaught of “crisis!” op-ed screeds published in newspapers. There were no countless hours of talking heads tut-tutting and painting doomsday scenarios.
It was passed by the Parliament and accepted by the people as striking the right balance.
No safeguards at all in many cases
And that’s it: the sum-total of safeguards to refuse life-saving medical treatment in Victoria. However, if the patient refuses medical treatment verbally, there are no mandated safeguards at all in either old or new Act, because the statutory safeguards apply only to refusal given in writing.
Yet despite all this, Messrs Sneddon and Rodrick rail against safeguards against coercion and elder abuse only in regard to the Voluntary Assisted Dying Bill, in which the safeguards are of a significantly higher calibre, with, for example, mandatory multiple doctor opinions, documentation trail, multiple requests, no go-ahead until approval by an external authority, notifications of numerous kinds, oversight by a specially-established panel, and so on.
It’s obvious what a flip-flop Messrs Sneddon and Rodrick’s demands are in respect of decisions that will foreseably result in death.
Another embarrassing flip-flop
Messrs Sneddon and Rodrick particularly also complain at length at the supposedly ‘lax’ definition of decision-making capacity in the Voluntary Assisted Dying Bill.
That’s a major and embarrassing flip-flop. Here’s why.
The section of the Voluntary Assisted Dying Bill that stipulates those requirements (Section 4) is the same section number 4 that governs the right to refuse of life-saving medical treatment in the Medical Treatment Planning and Decisions Act 2016. Only a few words have been changed to alter the context from refusal of treatment to consideration of assisted dying. Otherwise, the Sections are identical.
Messrs Sneddon and Rodrick don't point this out in their opinion piece. Indeed, I was unable to find online any evidence that they had published any complaint about the provisions when the Medical TreatmentPlanning and Decisions Act was in debate, nor since. If they have, I’d be happy for them to point it out.
Is it all a strategic ruse, anyhow?
It’s pertinent to ask if the objections are a ruse anyhow, because, as Andrew Denton has rightly pointed out, a key opponent strategy is not to give an outright “no” to assisted dying Bills, but to say only “not this Bill” and create an atmosphere of FUD (fear, uncertainty and doubt) so that it is defeated.
A typical ruse example
By way of example, I’ve published an account of how Victorian MP Daniel Mulino published outrageous misinformation about assisted dying. As a result, we had an extended conversation, during which he acknowledged that he had indeed published misinformation. At the end of the conversation I asked if he could support the Government’s Voluntary Assisted Dying Bill. (He’s a member of said Government.)
No, it’s too liberal, he said, pointing to Oregon’s Death With Dignity Act, now in force for nearly 20 years, as a more conservative approach. So I asked him if he would support a Bill like Oregon’s.
No, he said, there were still concerns about it.
By now you’ve spotted the merely incremental withdrawal of supposed possible support. So I asked him outright if there was any form of assisted dying Bill he could support.
The relevant word within a long discourse: No.
And there’s the answer that belies the political strategy. It doesn’t matter one whit what provisions are included in an assisted dying Bill, just criticize a bunch of provisions and create FUD to defeat it.
A direct challenge to Messrs Sneddon and Rodrick
If “doubters of this Bill” are genuine about permitting assisted dying in some defined circumstances, the duty is on them to define those circumstances and recommend wording to enact it.
And that’s the challenge I throw down directly to Messrs Sneddon and Rodrick. Don’t just bitch and gripe: define precisely what provisions and wording you think would be acceptable.
If you fail to stipulate what you deem acceptable, then your opposition to “this flawed Bill” is, like the supposedly ‘soft’ opposition of other campaigners in the negative, merely a ruse.
And that’s rather suggested by your deliberate use of the term “killing” for what most Australians believe to be an understandable and welcome release. But let’s give you the benefit of the doubt… for now.
Will you rise to the constructive challenge, or lurk in the shadows merely making snide remarks and flip-flopping?
----
* Section 62 of the Act also requires a doctor to notify the Public Advocate if “significant treatment” is refused — but only if it is refused by a substitute decision maker on behalf of the patient: not by the patient herself. And “significant treatment” is defined as treatments (not non-treatments) which are likely to have a serious impact on the patient (bodily intrusion, risk to life, side effects or distress). “Significant treatment” in the Act does not mean treatment whose refusal may result in death.
Blog by Neil FrancisPosted on Sunday 16th October 2016 at 12:03am
Wesley Smith and 'intelligent design' at the Discovery Institute
The Discovery Institute's Wesley Smith is at it again. In his latest anti-assisted-dying tirade published by LifeNews.com, he promote lies about the Dutch Groningen Protocol, despite my published detailed analysis — of how that regulation actually works in practice — providing ample evidence to disprove Mr Smith's polemic theories.
Creationism…with lipstick
Wesley Smith is a Senior Fellow at the Discovery Institute (DI). That's the organisation that promotes ‘human exceptionalism’ (the concept that humans are theologically pre-eminent in the universe), opposes the foundations of evolution, and controversially attempted to have ‘intelligent design’ taught as science in Pennsylvania public schools. The Pennsylvania District Court tossed out DI's ‘intelligent-design-as-science’ argument on the basis that:
“Teaching intelligent design in public school biology classes violates the Establishment Clause of the First Amendment to the Constitution of the United States (and Article I, Section 3, of the Pennsylvania State Constitution) because intelligent design is not science and ‘cannot uncouple itself from its creationist, and thus religious, antecedents.’” — Middle District Court of Pennsylvania
Intelligent design is, after all, merely creationism…with lipstick.
“Although technically illegal, infanticide happens regularly in Netherlands without legal consequence, and a bureaucratic checklist was published that determines which babies can be killed. Showing the direction of the current, the Groningen Protocol§ (as it is known) was published with all due respect and without criticism, in the New England Journal of Medicine.” — Wesley Smith
Mr Smith does nothing but parade astonishing ignorance and bias with this statement.
The facts
From my extensive and detailed research about the Groningen Protocol published in the Journal of Assisted Dying, Mr Smith ought to know that:
Neonatal euthanasia occurs around the world whether it is regulated or not. It occurs, for example, in France, where there is no protocol and no adult assisted dying law, at a rate far higher than the Netherlands.
The Groningen Protocol is lawful in the Netherlands and has recently been overhauled and further strengthened.
Its provisions are considerably more strict than are those of the Dutch euthanasia Act for decisionally-competent minors and adults.
In the nine years since the Protocol came into effect, there have been just two cases of neonatal euthanasia, both for cases of Herlitz type epidermolysis bullosa, a fatal and untreatable illness characterised by extreme internal and external blistering.
That compares with twenty two cases, mostly in relation to spina bifida, in the nine years prior to the Protocol coming into effect.
The Protocol was subject to considerable criticism from opponents when it was first published in the New England Journal of Medicine (NEJM).
Mr Smith has been criticised before by others for selectively using evidence and being:
"prepared to bend the truth to make a point, turn a stomach, and potentially radicalize a reader." — Matthew K. Wynia and Arthur Derse, Medscape
Perhaps Mr Smith doesn't care for the facts getting in the way of a good polemic? While he's entitled to his opinions, by repeatedly bending the truth and making statements contrary to the readily-available evidence, I argue that Mr Smith directly undermines any apparent 'authority' he claims for his musings.
Conclusion
The recurring pattern of resorting to misinformation reveals a lack of any real argument. I challenge Mr Smith to lift his game or retire his quill.
----- § Mr Smith links ‘Groningen Protocol’ to a blog published by the Euthanasia Prevention Coalition which is run by Canadian Catholic Alex Schadenberg. That blog is in turn based on a blog published by the Catholic online blog Mercatornet. The Mercatornet blog is itself a reproduction of an article by Dr Felipe Vizcarrondo who was a Clinical Bioethicist at Georgetown University (a Catholic and Jesuit institution), and which was originally published in Linacre Quarterly, the journal of the USA Catholic Medical Association.
Blog by Neil FrancisPosted on Sunday 8th May 2016 at 9:48pm
Jeanne Smits' completely false statement in LifeSiteNews
Well it didn't take long. Recently I posted a fact-based report card on Dutch euthanasia practice, based on the actual data from the 2015 annual report (and all the earlier reports) of the Dutch Euthanasia Commission. Now, just a few days later, conservative religious opponents have begun publishing completely untrue statements about Dutch euthanasia practice.
Catholic blog LifeSiteNews' 'Paris correspondent' Jeanne Smits has bolted out of the misinformation blocks, assertively and categorically stating in respect of the small increase in number of euthanasia cases from 2014 to 2015, that:
"The rise is mainly due to the increase of euthanasia for demented, elderly people as well as psychiatric patients, two categories that raise even more questions than 'ordinary' euthanasia for untreatable physical pain."
Smits goes on to correctly report that dementia was an underlying factor in 109 of the cases in 2015 (against 81 in 2014) and psychiatric disorders in 56 patients (against 41 in 2014).
The total number of euthanasia cases increased from 5306 in 2014 to 5516 in 2015, an increase of 210 cases. The increase in dementia cases was 28 and in psychiatric disorders was 15. Therefore, underlying dementia accounted for 13% of the increase, and psychiatric disorders 7% of the increase.
Cherry-picking
Smits has cherry-picked just the dementia and psychiatric illness figures and presented them in a way that supports her story arc, painting a bleak picture.
But by no stretch of the imagination does dementia and psychiatric illness account "mainly" for the increase as she categorically states.
What didn't Smits report at all? Cancer: the Netherlands' leading cause of death. In 2015, cancer was the underlying condition in 4000 euthanasia cases, against 3888 in 2014, a rise of 112 cases or 53% of the increase. That compares with dementia at 13% and psychiatric illness at 7% (20% combined), which Smits selectively critiques as a 'sharp rise'.
In no way is Smits' statement true.
No, let's be frank: it's an outright lie. Cancer was the major underlying condition accounting for more than half of the small increase (4%) of cases in 2015.
More evidence refutes the claim
Comparing one years' data with just the preceding years' data can be misleading when the number of observations is low, as it is for dementia and psychiatric illness euthanasia cases. Fortunately, we have data for more than just the one year.
Since 2012 the Euthanasia Commission has consistently published specific figures for dementia and psychiatric illness cases, so we can compare a rise over four years rather than just one. On this basis as a proportion of total 2012 cases, there has been a 17.9% increase in cancer-related cases, a 1.6% increase in dementia cases, and a 1.0% increase in psychiatric illness cases.
Longitudinal data is even more clear than a single year. It unequivocally refutes Smits' silly claim.
Bull is spread
Does Smits' claim matter much? Won't it just slip into oblivion?
No. Michael Haverluck of the conservative Christian paper OneNewsNow has already picked up Smits' article and repeated her claim as gospel. It remains to be seen how many other anti-euthanasia bloggers republish this nonsense.
Unacceptable conduct
In my view, publishing such a categorical yet false statement — even when unintentional — without first properly checking the facts, is unacceptable conduct. The article (and its derivatives) ought to be withdrawn.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
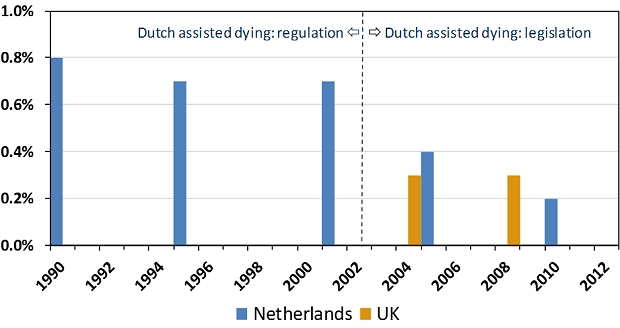
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.
Blog by Neil FrancisPosted on Sunday 15th November 2015 at 2:38am
ABC TV's Q&A panel discusses assisted dying law reform on 9th Nov 2015
In a recent opinion piece in the ABC’s Religion and Ethics section, Bernadette Tobin1 rails against assisted dying, commencing with the criticism that the ABC’s Q&A discussion on the subject this week “lacked precision.” But Tobin’s opinion piece itself commits exactly this offence, as I explain.
For the sake of brevity I’ll only quickly mention that Tobin’s piece also fails on the score of accuracy. For example, she wrongly asserts that “euthanasia” means a doctor administering lethal medication to a patient. It doesn’t. “Euthanasia” simply means “good death”: nothing more and nothing less, regardless of how it occurs. Tobin also asserts that voluntary euthanasia in lawful jurisdictions has caused non-voluntary euthanasia to develop. This is the polar opposite of published empirical research evidence.
But back to precision. Tobin employs two imprecise and deeply flawed arguments in her objection to assisted dying. She variously rolls them in together, so let’s unpack what they are: (A) the “it’s only fair” slippery slope, and (B) “it’s OK if you don’t mean it”.
A: The “It’s only fair” slippery slope
Tobin directly links assisted dying for the terminally ill to “anyone who is in pain, discomfort, constipated, incontinent, depressed, anxious and so on” by way of potential “benefit”. She conjectures that increasing the restrictions to who may qualify, and the process of qualification, would then be “unfair” to these others. She then goes on to extend the argument to those lacking in decisional capacity such as infants and those with Alzheimer’s. Surely, she says, “it would be ‘unfair’ to deny these people the ‘benefit’ that we will make available to those who are able to request it?”
Slippery slope indeed. And it’s wrong. Let me illustrate how, using a topic familiar in political debate over recent years: same-sex marriage.
Opponents of same-sex marriage law reform, when using arguments of the kind Tobin offers (as they often do), say that we can’t allow two men to marry, or two women to marry, because then we would have to allow three or more people to marry. Further down the slippery slope, we would have to allow people to marry animals. Don’t laugh: such things have been argued.
Next—given that under the Corporations Act 2001 (Cth), companies, owners’ corporations and incorporated associations are at law ‘persons’, and now that persons may marry—it would be “unfair” (note that I’ve used imprecision quotation marks around the word as Tobin does) to disallow people from marrying companies and companies from marrying each other.
Finally, using Tobin’s own line of argument, it would be “unfair” to deny infants and those with Alzheimer’s being married off for the alleged “benefit” (those quotation marks again) that everyone else is enjoying, so we must as an unavoidable consequence of the first step of allowing same-sex marriage, allow arranged marriages for babies and those with advanced dementia.
By now it’s easy to spot two terminal flaws in Tobin’s argument.
Firstly, the use of just one criterion (“fairness”—which she leaves imprecisely undefined) as the sole basis for decision making about this legislative reform is indefensible. What about other critical factors such as well-informed, rational, decisional capacity, judging and weighing what a “benefit” is, in the face of intolerable and unrelievable suffering, consistent with one’s own values and beliefs, who may decide, and the right not to participate?
Secondly, any slippery slope’s purported summit (from which changes are argued only to slip downwards) is deeply rooted in the normativity of the present. We are used to marriage being between a man and a woman. In our relative comfort we accept it as ‘normal,’ ‘good’ and the ‘right thing’.
In decision-making scholarship this normativity is known as “anchoring”. Like an anchor around which a boat will swing according to the wind and tide, we take the pivot point (the anchor of the now), as the natural starting point for future decisions, comparing changes only to the present state of affairs.
But it isn’t a valid anchor, and assuming that it is seriously biases our thinking. We need cast our anchor back just one mooring from the current point to see how the anchor tints our decision-making spectacles:
“We can’t allow a man and a woman to marry, because then it would be unfair to not allow two men to marry, or two women to marry, and then…”
Clearly, it is imperative that we outlaw marriage altogether.
The upshot of this slippery slope, when followed properly to its own logical conclusions, is that we must deny all rights because we can confect a slippery slope into a hypothetical moral abyss for any right.
B: It’s OK if you don’t mean it
Tobin further argues that relieving distressing symptoms “is good palliative care, even when that relief happens to hasten death.”
She doesn’t name it explicitly, but this is the doctrine of double effect, an argument first crafted in the thirteenth century by Catholic priest Thomas Aquinas. The doctrine suggests that a bad consequence of an action is justifiable if the agent did not intend the bad effect, if the intended good effect outweighs the bad effect, and if the agent applies diligence in attempting to minimise the bad effect. Notice that the doctrine speaks directly about the intentions of the agent and is silent on the views of the person upon whom the agent might act.
Tobin rails against a doctor intentionally administering a lethal dose to a patient (regardless of whether it is the dying patient’s most fervent wish) and slams the expressions “dying with dignity” and “aid in dying” as “fudges”.
Yet the doctrine of double effect, for which she argues in support, is itself a fudge because it says:
“It’s OK to for a doctor to decide to and actually kill their patient (after all, they hastened the patient’s death), as long as they don’t mean to, and they mean well.”
What kind of standard is the secret stuff that goes on inside a doctor’s head without reference of any kind to the patient’s own views and desires, when compared to a fully informed, documented and tested request from the patient?
It’s no wonder that many scholars (as do I) consider the doctrine of double effect problematic.
--
Bernadette Tobin is the Director of the Plunkett Centre for Ethics, a joint initiative of St Vincent’s Hospital, Sydney, and Australian Catholic University (ACU). According to ACU, a core mission of the Centre is to “bring a Catholic perspective to all its endeavours”.2
It’s unsurprising then that I detected neither broad thrust nor any detail of Tobin’s ABC opinion piece that deviated from the views of the Vatican. So be it.
There are many points on which Tobin and I agree, such as the potential benefits of palliative care for the dying. I argue, though, that basic scrutiny of the proffered 'principles' reveal them as deeply flawed and unpersuasive.