Blog by Neil FrancisPosted on Thursday 27th July 2017 at 11:52pm
Research results must be judged in relation to the study's methodology.
In his latest blog, titled “Who are you going to trust?”, anti-assisted dying lobbyist Mr Paul Russell says:
“Polling noted today in the Australian shows a significant level of distrust in our political classes to get the issue of euthanasia and assisted dying right.”
He then goes on to quote some select statistics from said poll. In his blog, he mentions nothing about the sponsorship or conduct of the poll. After some searching, I found no other reference to said poll on his ‘HOPE’ website.
This is rather curious, because The Australian article he quotes, points out that the ‘poll’ was commissioned by him (his website is called ‘HOPE’).
Thus, Mr Russell tries to add credibility to his ‘poll results’ in his blog by citing only that it has been reported in a national newspaper. This ‘quote-someone-else-so-it-must-be-authoritative’ rhetorical strategy has been used before by opponents of assisted dying (see Box at end).
But as Mr Russell has himself promoted — happily republishing the opinion of the CEO of Christian Medical Fellowship (UK) — “opinion polls add up to very little.” That’s quite true… when they’re poorly designed and run, including the big no-no, ‘push-polling’, in which the researcher attempts to get the answer they want by crafting questions more likely to get it.
I searched hard for any reference to the methodology of said ‘poll’, but was unable to identify any despite a diligent search. Therefore, we don’t know what approach Mr Russell took: robust or otherwise.
Let’s assume for the sake of argument (and the absence of public evidence) that a poll of some kind was actually conducted. If it were a truly legitimate poll, you’d think that Mr Russell would be shouting about the study from his own rooftop (the ‘HOPE’ website). But so far, he hasn’t.
Mr Russell, while quoting statistics, has said absolutely nothing about the methodology — that I can find via a quite diligent search.
Results can only be interpreted in light of how the research was actually conducted, so quoting a 'study' while failing to publish its methodology in full is an absolute no-no. It only invites derision.
Rebecca Urban, for The Australian, quotes a number of ‘statistics’ from the ‘poll’ seemingly without question. But she’s hardly to blame: she’s skilled at journalism, not primary research.
So, for the benefit of Paul Russell, Rebecca Urban and all journalists reporting claimed statistics, here’s your minimum standard of conduct if the public are not to guffaw at the claims. All reported results must be in relation to properly disclosed methodology:
Who commissioned the research? (✔ Ms Urban reports who)
Who conducted — actually carried out — the research (e.g. a reputable research company)?
What precise population were respondents drawn from, how were they recruited, and screened in or out? What were the counts and percentage participation (approached/participated)?
What were the dates of the fieldwork?
What procedures were used to establish and maintain the authenticity of who was sampled (e.g. if an online poll, could people from anywhere technically participate in this Victorian poll)?
How was the questionnaire administered (e.g. paper self-complete, online, CATI)?
What was the script of stimuli administered to respondents? In other words, what prompts were given and what questions were asked: exact order and wording?
What results were obtained for each question (i.e. full rather than selective crosstabs)?
Until Mr Russell publishes in full how his ‘poll’ was conducted, the only honourable course of action for him to pursue is to withdraw the claimed results.
Until then, we can only see them as untrustworthy and a bit of a joke.
Rhetorical tactic — “Not” quoting yourself
This rhetorical tactic is also used by Mr Russell’s fellow Catholic, Prof. Margaret Somerville. For example, in her 2015 book Bird on an Ethics Wire, in relation to the supposed (but fanciful) fear of being euthanized in the Netherlands if adequate pain management is accepted, Somerville says in Chapter 4:
“It has been alleged that Dutch physicians have interpreted patients’ consent to pain management as consent to euthanasia.38”
If you’re like most people, you’d assume, given the effort of a citation (38), that an independent source had made the statement based on some evidence. Indeed, if you look at reference 38 you’ll see that the author is Lauren Vogel, and the source article is in the Canadian Medical Association Journal. All sounds like solid, legit stuff, doesn’t it?
However, Ms Vogel is a journalist, not a Dutch medic or a researcher, and what she reports in relation to Somerville’s claim is merely a quote of what someone said. And who is that someone? Why, it’s Margaret Somerville — what a coincidence!
Somerville could have just said “I’ve argued this before…”, but instead gives a seemingly robust reference to a source that has the appearance of independence and scholarship. Yet obviously she knows that the source is merely herself saying so.
Let’s be clear: something is not true just because someone alleges it. Even if they allege it twice or more. And happen cite themselves via someone else in the process.
Blog by Neil FrancisPosted on Friday 21st July 2017 at 1:53am
The Parliament of Victoria, Australia
The Victorian Government has introduced its assisted dying Bill into the Victorian Parliament. It's based on extensive consultation with a wide range of stakeholders, and over 1,000 submissions. You can read all about it here.
The Ministerial Advisory Panel on voluntary assisted dying today handed down its final report to the Government.
The Panel was comprised of seven subject experts, with Professor Brian Owler as Chair and Professor Margaret O'Connor as Deputy Chair.
It consulted extensively across Victoria, taking hundreds of submissions and appearances from relevant stakeholders, and reviewing legislation from other jurisdictions in which one form or other of assisted dying is permitted.
Today, it formally handed its report, comprising over 250 pages, to the Government.
The Panel has developed what is arguably the world's most detailed and carefully laid out principles to inform legislation, and are a credit to its efforts and professionalism.
Key aspects of the recommendations for voluntary assisted dying are:
The person must be 18 years or over; and
Be ordinarily resident in Victoria and an Australian citizen or permanent resident; and
Have decision-making capacity in relation to voluntary assisted dying; and
Be diagnosed with an incurable disease, illness or medical condition that:
is advanced, progressive and will cause death; and
is expected to cause death within 12 months; and
is causing suffering that cannot be relieved in a manner the person deems tolerable; and
Doctors and other healthcare workers are not permitted to raise assisted dying — only to respond to formal patient requests.
The person must make three formal requests, the second of which must be written and witnessed by two independent people.
The person must make the request themselves. Nobody else is authorised to make the request, and the request cannot be made via an advance care directive.
Ordinarily, the minimum timeframe between first request and opportunity to take the medication is ten days.
The person must maintain decisional capacity at all three requests.
Two doctors must reach independent assessments that the person qualifies.
Only doctors who have completed specialist training for voluntary assisted dying may participate.
Any healthcare worker may decline to participate for any reason, without penalty.
A prescription dispensed for the purpose of voluntary assisted dying must be kept in a locked box and any unused portion returned to the pharmacy after death.
The person must self-administer the medication; except if the person is unable to, a doctor may administer. An independent witness is required if the doctor administers.
Establishment of an authority to receive assisted dying reports, to assess reports, and to refer unacceptable cases to disciplinary or prosecutorial authorities.
For Parliament to review summary reports; twice in the first two years and annually thereafter; a formal review at five years.
In total, the recommendations include no fewer than 68 safeguards, designed to strike, uniquely for Victoria, an appropriate balance between access to the law, and protection of dying persons.
The Government will respond to the Final Report shortly, and it is anticipated that legislation will be introduced into the Victorian Parliament in August or early September.
A full copy of the Final Report can be obtained here.
-----
Safeguards proposed for Victoria's voluntary assisted dying framework
Access
Voluntary
Limited to 18 years and over
Residency requirement [Victorian resident and Australian citizen or permanent resident]
Limited to those with decision-making capacity
Must be diagnosed with condition that meets restrictive set of criteria [advanced, progressive and will cause death]
End of life is clearly defined [death expected within weeks or months, not more than 12 months]
End of life condition combined with requirement for suffering
All of the eligibility criteria must be met
Mental illness alone does not satisfy the eligibility criteria
Disability alone does not satisfy the eligibility criteria
Request
Must be initiated by the person themselves
No substitute decision makers allowed
Cannot be included as part of an advance directive
Health practitioner prohibited from raising voluntary assisted dying
Person must make three separate requests
Must have written request [witnessed in the presence of a medical practitioner]
Two independent witnesses to request [exclusions for family members, beneficiaries, paid providers]
Specified time must elapse between requests [first and third requests must be at least 10 days apart with exception when death imminent]
Additional time required to elapse between steps of completing process [second assessment and third request must be at least one day apart
Must use independent accredited interpreter [if an interpreter is required]
No obligation to proceed, may withdraw at any time
Assessment
Eligibility and voluntariness assessed by medical practitioners
Must be two separate and independent assessments by medical practitioners
Assessing medical practitioners must have high level of training/experience
Assessing medical practitioners must have undertaken prescribed training [to identify capacity and abuse issues]
Requirement to properly inform person of diagnosis, prognosis and treatment options, palliative care, etc, [by both assessing medical practitioners]
Referral for further independent assessment if there is doubt about decision-making capacity
Coordinating medical practitioner must confirm in writing that they are satisfied that all of the requirements have been met
Medication management
Person required to appoint contact person who will return medication if unused
Medical practitioner must obtain a permit to prescribe the medication to the person
Medication must be labelled for use, safe handling, storage and disposal
Pharmacist also required to inform the person about administration and obligations
Medication must be stored in a locked box
Administration
Medication must be self-administered [except in exceptional circumstances]
If physical incapacity, medical practitioner may administer
Additional certification required if administered by medical practitioner
Witness present if medical practitioner administers
Practitioner protections
Health practitioner may conscientiously object to participating
Explicit protection for health practitioners who are present at time of person self-administering
Explicit protection for health practitioners acting in good faith without negligence within the legislation
Mandatory notification by any health practitioner if another health practitioner acting outside legislation
Voluntary notification by a member of the public of a health practitioner acting outside legislation
Mandatory reporting
Reporting forms set out in legislation
Reporting mandated at a range of points and from a range of participants to support accuracy
First assessment reported [to Board]
Second assessment reported [to Board]
Final certification for authorisation reported [to Board, incorporates written declaration and contact person nomination]
Additional form reported [to Board] if medication administered by medical practitioner
Prescription authorisation reported by DHHS [to Board]
Dispensing of medication reported [to Board]
Return of unused medication to pharmacist reported [to Board]
Death notification data reported [to BDM and collected by Board]
Offences
New offence to induce a person, through dishonesty or undue influence, to request voluntary assisted dying
New offence to induce a person, through dishonesty or undue influence, to self-administer the lethal dose of medication
New offence to falsify records related to voluntary assisted dying
New offence of failing to report on voluntary assisted dying
Existing criminal offences for the crimes of murder and aiding and abetting suicide continue to apply to those who act outside the legislation
Oversight
Guiding principles included in legislation
Board is an independent statutory body
Board functions described in legislation
Board reviews compliance
Board reviews all cases of [and each attempt to access] voluntary assisted dying
Board has referral powers for breaches
Board also has quality assurance and improvement functions
Board has expanded multidisciplinary membership
Board reports to publicly [to Parliament every six months for first two years, thereafter annually
Five year review of the legislation
Guidelines to be developed for supporting implementation
To add insult to injury, it flip-flops on its stance.
Never mind that the argument is contradicted by evidence
The Church’s favourite argument — already contradicted by scholarly analysis that curiously seems to be of no interest to the Church — is this: if people are given the choice of assisted dying, they will feel compelled to choose it, coerced by doctors, greedy relatives or others; subtly or otherwise.
No matter that health care workers routinely report that relatives usually try and persuade their dying loved one to endure yet another invasive and burdensome treatment; not dissuade them from it.
The flip-flop
If the Catholic Church were indeed genuinely concerned about coercion of ‘the vulnerable,’ then it would equally oppose the right to refuse medical treatment, particularly if the treatment were life-prolonging. But it doesn’t.
If granny might die as a result of refusing a particular medical intervention, then a doctor might persuade her to refuse in order to conserve medical resources. Or greedy relatives might persuade her so that they are relieved of the burden and expense of looking after her and gain earlier access to her estate.
As eminent legal scholar Gerald Dworkin has argued,1 if there’s a theoretical ‘slippery slope’ for assisted dying, it’s the same for the refusal of life-preserving medical treatment.
To hold different positions under the same risks is to flip-flop. That’s especially so when there are numerous safeguards built into assisted dying statutes, but currently few or none for the right to refuse life-preserving medical treatment.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
Local experience confirms risk is theoretical
In my home state of Victoria, where the right to refuse any unwanted medical treatment has been enshrined in statute for nearly three decades (the Medical Treatment Act 1988), how many prosecutions have there been under the Act’s provisions against inappropriate persuasion?
Precisely none. Not a single case. So much for the theory.
It all serves to highlight that the Catholic Church’s only real argument is that it believes that it’s morally wrong to deliberately hasten death. However, it avoids this argument because as a religious tenet, it doesn’t appeal to the masses.
Catholic directives
The Church’s flip-flop about ‘the vulnerable’ is not a one-off accident. Take for example the ‘Ethical and Religious Directives for Catholic Health Care Services’ published by the United States Conference of Catholic Bishops.2
The Bishops ‘direct’ that there is no obligation on patients to use disproportionate means of preserving life. They state that disproportionate means are:
“…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
The Bishops further ‘direct’ that:
“The free and informed judgment made by a competent adult patient concerning the use or withdrawal of life-sustaining procedures should always be respected and normally complied with, unless it is contrary to Catholic moral teaching.”
Setting aside the Church’s hubris of dishonouring the patient’s choice if the Church disagrees, it would be theoretically easy for someone to persuade the patient that hope was not reasonable, that the burden would be too great, or that the cost to the family or society would be too high.
Suffering for our God’s (your own) good
On the next page, the Bishops expressly ‘direct’ that:
“Patients experiencing suffering that cannot be alleviated should be helped to appreciate the Christian understanding of redemptive suffering.”
That’s unqualified. So, if you’re atheist, agnostic, Jewish, Hindu, Muslim or even a Christian who believes assisted dying can be appropriate, as a patient in their institutions you are to be persuaded that suffering against your beliefs and wishes is ‘redemptive’ in the eyes of the Vatican’s version of a God.
In Australia in 2009, for the Office for Family and Life in the Catholic archdiocese of Adelaide, Mr Paul Russell argued in News Weekly that “there is a point to suffering” because:
“It’s about the profound connection that each and every life has to the incarnate God … We know that the sufferings we endure well are joined in some mysterious way to the sufferings of Christ.”
Pity any poor soul who doesn’t share Mr Russell’s views. Curiously, there is no mention of this underpinning belief in his anti-assisted dying blog, “HOPE.”
Invalid argument in any case
The Church’s argument that ‘the vulnerable’ will be ‘at risk’ from assisted dying laws — for example in the Victorian Bishops’ recent pastoral letter to the Catholics of Victoria opposing the upcoming assisted dying parliamentary Bill — is itself fundamentally invalid.
That’s because, as I’ve previously explained, it’s a circular argument: a logical fallacy.
A circular argument: We must ban yellow socks on Wednesdays or the 'vulnerable' will be 'at risk'.‘The vulnerable,’ by definition are those ‘at risk,’ and will still be so if we wear yellow socks on Wednesdays. Therefore, we should ban such bright footwear midweek — and anything else we happen to oppose — on the same basis.
Might anyone suggest that “we should ban religion because the vulnerable will be at risk of succumbing to extreme religious views”?
Will the Church change its mind?
The Catholic Church does change its mind from time to time, though its reforms are glacially slow.
Take, for example, its theory of limbo, a place on the doorstep of hell where, the Church claimed, babies go if they die before they’re baptised: that they’d be prevented from entering heaven. It would be hard to imagine a crueller worry to put into the heads of uneducated new parents.
But in 2007, after centuries of confidently promoting the theory, the Catholic Church decided that it was wrong and buried it.
Will it change its mind on assisted dying? Maybe, but don’t hold your breath.
Conclusion
The Catholic Church, reeling from its extensive failure to protect our most vulnerable — children — and notwithstanding some good individuals within, still presumes to morally lecture the rest of us with the logical fallacy of how ‘risky’ assisted dying legislation is supposed to be to ‘the vulnerable,’ while flip-flopping in support of refusing life-saving medical treatment under the same theoretical risk.
The Bishops’ rhetoric amply exposes their confected crisis against assisted dying as nothing but religious doctrine draped in faux secular garb… in reality a sheep in wolves’ clothing.
References
Dworkin, G, Frey, RG & Bok, S 1998, Euthanasia and physician-assisted suicide, Cambridge University Press, Cambridge, New York. pp.66ff
Blog by Neil FrancisPosted on Tuesday 13th June 2017 at 2:38am
The Age reports a 'gloves off' campaign of misinformation
Both the Herald Sun and The Age reported last week that religious anti-assisted dying crusaders are running a 'gloves off' campaign in Victoria.
Religious forces are gathering once again to attempt to thwart the views of the great majority of Victorians in favour of assisted dying law reform.
Matt Johnston in the Herald Sun quoted Paul Russell, a long-term figure in Catholic circles, and Greek Orthodox Bishop Ezekiel, in statements against assisted dying.
Farrah Thomazin in The Age quoted religious stalwarts Margaret Tighe of Right To Life, and the Australian Christian Lobby, in further statements against assisted dying.
The crux of the story is that 'pollsters' claim to have run a survey in Victoria. They refuse to be identified. They refuse to publish their methodology. And they refuse to publish all their results. Enough said.
They cherry-pick an item from their supposed poll to claim that 33% of Victorians who oppose assisted dying will change their vote against a supporting politician at the next election. They neglect to mention that only a tiny minority of Victorians actually oppose assisted dying. Their analysis is astonishingly superficial, even assuming they ran a proper, robust poll and didn't manufacture the numbers themselves.
They then use this tidbit of 'data' to put the fear of electoral defeat into politicians who will soon to face an assisted dying Bill in the Victorian Parliament.
What rubbish. Assisted dying (AD) opponents seem to be utterly shameless in misrepresenting and distorting cherry-picked data to push their religious agenda — which they pretend isn't religious.
The real situation in respect of AD is the exact opposite of their claims as I show in a proper, robust analysis of legitimate data, demonstrating that:
A massive 78.9% of Victorians support AD, with only a tiny 8.1% opposed. Strong supporters outnumber strong opponents by more than ten to one.
Significantly more supporters of AD believe that law reform is personally important, than opponents believe the status quo (no law) is personally important.
At a general election, far more Victorian voters will punish Members who oppose the AD Bill than will punish Members who support it (3.5 to 1 overall, 2.4 to 1 for the Liberal/National Coalition and 6.6 to 1 for Labor).
The co-sponsors of Victoria’s 2008 AD Bill were returned with greatly increased majorities (including relative to their party’s overall performance) despite campaigns against them by anti-AD crusaders.
So that Victorian politicians are not misled, I have forwarded my report to the Victorian Government's Cabinet and other selected members of Parliament.
The only way in which this campaign could be called 'gloves-off' is that opponents, lurking around with their shadowy misinformation, don't want to get bullshit on their mittens. Hands seem to be much easier to wash. And hide.
Fact file by Neil FrancisPosted on Thursday 25th May 2017 at 12:00am
Those actively opposing assisted dying laws are Australia's most religious. Photo: Donaldytong
A claim was recently made on ABC’s QandA that at least 70% of Catholics and Anglicans support assisted dying. The claim was challenged and a FactCheck prepared and vetted by scholars. They concluded that some but not all polls supported the statement. I show unambiguously that relevant polls do. I show further, as I have in the past, that opposition is largely associated with Australia's most religious.
In 2007, a Newspoll survey found that 74% of Catholics and 81% of Anglicans support assisted dying. The 2016 Australian Election Study (AES), run by scholars at Australian National University, found almost identical rates: 74% of Catholics and 79% of Anglicans. Although a majority of all religious denomination groups support assisted dying, opposition is highest among minor Christian denominations (Figure 1).
Figure 1: Attitudes toward assisted dying by major religious denominations Source: AES 2016. Note: Chr. = Christian
A significant majority of support for assisted dying was also found across all age groups, education levels, income levels, states, and major political party affiliations and religious denominations, with support amongst Australians overall at 77%.
Casting doubt
However, another poll cited in the FactCheck found far less support: the 2011 National Church Life Survey (NCLS). It found just 28% of Catholics and 25% of Anglicans supported assisted dying.
The problem with the NCLS poll is that it didn’t take a valid sample of Australian Catholics and Anglicans. It sampled mostly or only those who frequently attend religious services.
Views vary widely by attendance frequency
Figure 2 shows the level of support amongst the Australian public, by frequency of attending religious services. While just 2.4% of those who never attend religious services oppose assisted dying, 46.1% of those attending at least once a week oppose it.
Figure 2: Attitudes toward assisted dying by frequency of attending religious services Source: AES 2016
NCLS poll cannot answer the question
The NCLS results were even more negative than the AES ‘at least once a week’ results. That’s explained by the NCLS methodology. Firstly, occasional attenders were underrepresented, and non-attenders were excluded altogether. Secondly, more church employees (the most deeply committed and aligned with church policies) than others would have participated. Thirdly, responders may have felt pressured to toe the church line because the survey forms were collected by the churches themselves. And fourthly, those who disagreed with the church line would be less likely to participate.
ABC QandA question answered
So we can discount the NCLS poll because it was not suited to answer the question about all Australian Catholics and Anglicans.
On that basis, it is not only reasonable to say that “up to 70% of Catholics and Anglicans support assisted dying,” but to say that “at least 70% of Catholics and Anglicans support assisted dying.”
Religious connections of opposers
But, back to the opposition of assisted dying. AES data shows that 92% of those opposing and 94% of those strongly opposing assisted dying have a religious affiliation (self-identify with a religious denomination) or attend religious services. So, while a tiny minority of opposers had no religious affiliation nor attended religious services, almost all those opposing have a religious connection.
Frequent service attendance entrenches opposition
If we focus in on those who identify with a religious denomination and who disagree with assisted dying, we find that there’s a massive difference in opposition to assisted dying between the ‘at least once a week’ attenders and everyone else (Figure 3).
Figure 3: Frequency of attending religious services amongst those with a religious affiliation and who disagree with assisted dying Source: AES 2016
Not only are the majority of opposers weekly religious service attenders, but weekly attenders are more likely to be strongly opposed. This highlights the strong alignment with and commitment to religious teachings, which (with rare exceptions) oppose assisted dying.
If we define the most religious Australians as those who attend religious services monthly or more often and who self-identify with a religious denomination (“Regulars” in Figure 4), and who make up just 15.7% of the population, their attitudes are remarkably more opposed to assisted dying than all other Australians — by a factor of more than eleven to one.
Figure 4: Attitudes by religious service attendance plus denomination affiliation (“Regulars”) Source: AES 2016
Amongst the 84.3% of Australians who are not “Regulars”, almost all of them (85.7%) agree with assisted dying, and almost none of them (3.6%) disagree.
Demographic differences explained by religiosity
The variation in attitudes toward assisted dying by general demographics is largely explained by religiosity — defined here as ‘the frequency of attending religious services’.
For example, the increased opposition amongst older Australians is explained by their increased religiosity. The same applies to religious denomination affiliation (e.g. Catholics attend services more often than Anglicans), education, urban versus rural residence, and political party first preference.
Religiosity was the only variable that independently explained variations in opposition to assisted dying.
The double whammy — affiliation and attendance
Also informative is the comparison of those with or without a religious affiliation versus those who do and don’t attend religious services. (Australians fall into all four categories.)
Amongst those with no religious affiliation, people who do attend religious services are only slightly less likely (than those who don’t attend) to support assisted dying (-7%), and their difference in attitude is mostly to neutrality.
However, of those with a religious affiliation, people who do attend religious services are significantly less likely to support assisted dying (-27%), and the majority of their difference in attitude is opposition rather than neutrality.
Thus, those more deeply aligned with their religious denomination through service attendance are significantly more likely to oppose assisted dying.
Moderated by personal experience
The 2007 Newspoll study asked respondents if they had personal experience of someone close who was hopelessly ill and had wanted voluntary euthanasia.
Amongst those with no religious affiliation, this personal experience increased support for assisted dying by just 3.7%, because support was already very high: from 90.9% to 94.6%.
However, amongst those with a religious affiliation, personal experience increased support for assisted dying markedly by 15.2%: from 72.4% to 87.6%.
Thus, those attending religious services, yet with close, personal experience of hopeless illness with a desire for assisted dying, were significantly less likely to align with opposed religious doctrine.
The most religious are a small minority
With so much opposition amongst Australia’s most religious, why is overall support for assisted dying so high? It’s because Australia’s most religious are a small minority of the population.
Nearly half (48%) of Australians never attend religious services, two thirds (65%) attend less than once a year or never, and three quarters (75%) attend once a year or less, including never.
Those who attend religious services frequently (weekly or more often) comprise just 12% of the population, while those who attend regularly (monthly or more often which includes the weeklies) comprise 16%.
Religion in Australia has been declining for decades, and the fall is likely to continue (see Appendix A of the full report, here), meaning that support for assisted dying is likely to increase in the future.
Conclusions
I’ve previously demonstrated how all the signatories to a major anti-assisted dying advertisement were deeply connected with religion. The AES and other studies further our understanding of wider public attitudes toward assisted dying in Australia. They show that while a substantial majority of Australians support assisted dying, almost all the opposition to it is connected with religion, particularly amongst the most religious who are a small minority of the population.
Despite the religious connection of those opposed, there is ample, robust evidence that a great majority of Catholic and Anglican Australians support assisted dying, backing the claim made on national television.
Clergy opposing assisted dying are not representing the broader views of their flocks. Perhaps they may not see that as their role, and perhaps this misalignment of attitudes and beliefs is an example of why religion in Australia is declining.
However, reflecting the views of the great majority of the constituency is the role of politicians, who would do well to take note of this robust evidence of a significant majority of support for assisted dying.
Blog by Neil FrancisPosted on Wednesday 19th April 2017 at 1:39am
Patricia Flowers calls Margaret Somerville's arugments 'bullshit' on national television. Photo: ABC
Last week, Mr Xavier Symons published a defence of Professor Margaret Somerville, whose arguments against assisted dying were called ‘bullshit’ by Patricia Flowers on the ABC’s Q&A program. Symons and Somerville are colleagues at the Institute for Ethics and Society at the Catholic Notre Dame University of Australia.
Mr Symons made an important point: that a law about restricted self-choice for assisted dying is in no way comparable to the Nazi Germany euthanasia (or more correctly, eugenics) programme. While Prof. Somerville agrees that such comparisons are invalid, she nevertheless often mentions Nazi Germany as a ‘question’ when debating assisted dying. That’s a bit of a fudge.
And Mr Symons, in his defence of Prof. Somerville, offers some fudges of his own. While Dr Iain Brassington has offered a cool philosophical examination of Mr Symons’ opinion piece in a Journal of Medical Ethics blog, I’ll provide more of an evidential analysis.
Wrong on Dutch law and practice
Mr Symons said that euthanasia was legalised in the Netherlands in 2002. While technically that may be true, it's misleading. Assisted dying was actually made lawful in the Netherlands in 1982, after considerable debate and a number of court cases, when the Board of Procurators-General (the highest prosecutorial authority) formalised a set of conditions under which doctors would not be prosecuted for helping a patient die.
In practice, wider physician participation commenced in 1984 when the Royal Dutch Medical Association (KNMG) issued its own guidelines for clinical practice, based on the Procurators-General ruling, and grew to more than a thousand cases a year by the late 1990s.
It was in 2002 — when the Termination of Life on Request and Assisted Suicide (Review Procedures) Act came into effect — that the Dutch law on assisted dying changed from regulatory to statutory.
Mr Symons also claimed that since 2002, the “Dutch legislation [has] changed several times.” That’s not true: in fact, not one word of the Act has changed since it came into effect.
Nor has there been a “steady rate of increase” in the Dutch assisted death rate since 2002 “even when there was no legislative change” as he claimed. There has been an increase, but far from ‘steady.’ Rather, it’s a sigmoid (stretched-S) curve with very little initial increase, then increasing, and then levelling out again. It’s a pattern typical of human behaviour adoption, and has occurred in both Belgium and the Netherlands.
Selective Euro-evidence
Mr Symons also claimed “significant evidence from Belgium, Netherlands, Luxembourg” for his argued slippery slope. Yet he quotes percentages for only the Netherlands, correctly noting that assisted deaths increased from 1.3% of all deaths in 2002 to 3.7% in 2015.
Mr Symons doesn’t mention that:
the Dutch assisted dying rate was lower for a number of years after 2002 than before — as physicians and the public were still getting to grips with the new Act;
the Netherlands’ assisted dying rate dropped between 2014 and 2015;
the rate in Belgium (1.8% in 2015) is half the Netherlands’;
the rate in the Flanders (Dutch) north of Belgium (2.5% in 2015) is higher than in the Wallonia (French) south (0.87%), suggesting that higher rates may be a characteristic of Dutch culture;
the rate in Luxembourg, with very similar legislation, is a tiny one twentieth of the Dutch rate — 0.18% in 2014 (the most recent year of available data); or that
there is no evidence to date of the rate increasing in Luxembourg.
Selective North American evidence
While Mr Symons reports the Dutch rate as a percentage of all deaths, he reports his only other figures (for Oregon) as raw counts: rising from 16 in 1998 (before which assisted dying was entirely illegal) to 132 in 2015. (Actually, the final figure for 2015 was 135 cases.) What he fails to mention is that the Oregon rate in 2015 was 0.38% of all deaths, just one tenth of the Dutch rate. That is, the percentage is far less ‘impressive’ to his thesis and raises questions about ‘inevitable slippery slopes.’
The increase is hardly surprising given that when conduct is made newly lawful, only a few people might pursue it in its first year, with more people pursuing it seventeen years later. Even then, one hundred and thirty-five cases out of nearly thirty-six thousand deaths is hardly a “normalisation,” as Mr Symons argues.
He also argues that Quebec’s initial figures are “alarming,” without reporting the rate as a percentage of all deaths. Data from the first year (2015–16) indicates a rate of 0.74%, slightly lower than French-speaking Wallonia in 2015 (0.87%). (Half-way through the 2015–16 period, Canada’s Federal Parliament also passed an assisted dying law.)
The latest comparative data
The latest data on assisted death rates in Benelux and North America is shown in Figure 1. As I explain in one of the most detailed comparative analyses of lawful assisted dying practice conducted to date, it is likely that the higher rates are associated with Dutch culture.
Figure 1: Assisted dying in Benelux and North America as a percentage of all deaths
Notes: Dutch cultures appear in orange. Flanders is the northern Dutch, and Wallonia the southern French, ‘half’ of Belgium.
Sources: Government statistics offices and assisted dying authority reports; Quebec, CBC News
The case of Vermont
In the USA state of Vermont (with an Oregon-like Act since 2013), a small number of people (38) have been prescribed lethal medication in the first three years. (Data is not available by year.) Assuming for the sake of argument that all of them took the medication (while Oregon and Washington data indicates that a third or more don’t), that would equate to an assisted dying rate of around 0.27% of all deaths as an annual average for 2013–15.
Don’t mention Switzerland
Switzerland is perhaps the most ‘inconvenient’ case for slippery slope hypotheses, which might explain why assisted dying opponents usually avoid mentioning it. It has the world’s oldest assisted suicide law, in effect since 1942. It is also the least prescriptive: the only specific statutory requirement is that any assistance rendered must not be for reasons of self-interest. That’s it.
Surely a law in effect for 73 years and devoid of all the complex requirements of others would be the foundation for an out-of-control assisted dying rate, much higher than the Netherlands at 3.7%?
It isn’t. In 2015, the rate for Swiss-resident assisted deaths was 1.4%. The rate including foreigners — in other words, with a global population of potential ‘slippery slope candidates’ — was 1.7%. That’s less than half the Dutch rate.
Conclusion
To summarise, the lawful assisted dying rate varies widely between cultures, currently by a factor of twenty. Yet there’s one thing consistent amongst them all: the most common reason for pursuing an assisted death is advanced cancer.
Ultimately, the only thing Mr Symons’ argument establishes is that he prefers to negatively describe any use of a law of which he disapproves as “normalisation,” regardless of its usage rate. If this were not true it would be incumbent on him to nominate a non-zero assisted dying rate that he thinks acceptable, but not “normalised.”
To be sure, I agree with Mr Symons that it’s important to “review the hard facts” around assisted dying.
And yet, when he promised the reader that his “valid slippery slope” argument would be based on “compelling empirical” evidence, he made incorrect or misleading statements, provided cherry-picked morsels of data, and wrapped it all up in a loaded assumption. I think that Patricia Flowers would call that ‘bullshit.’
The F filesPosted on Monday 27th March 2017 at 8:50pm
Dr Michael Gannon announces the AMA's policy review to AMA members in 2015
In 2016, the Australian Medical Association (AMA) reviewed its policy on ‘euthanasia and physician assisted suicide.’ Despite ample evidence to the contrary, the AMA executive set its policy as opposed to assisted dying, when the only position that would have acknowledged and respected the views of most of its membership was a position of neutrality.
The Australian Medical Association (AMA) has been historically opposed to legislative reform that would permit doctor-assisted dying for patients in unremitting and untreatable extremis. Its hostile position had been expressed through a Position Statement (PS) in effect for at least a decade, although its Code of Ethics has been completely silent on the matter.
The AMA’s opposition to doctor-assisted dying has been one of the factors leading to the failure of a number of attempts at assisted dying law reform.
In 2015 the AMA announced a review of its ‘policy’ on ‘euthanasia and doctor assisted suicide,’ managed through its Federal Council. The review was conducted from late 2015 and throughout 2016. It included an online survey of more than 3,700 Australian doctors.
Deeply flawed survey — against assisted dying
The survey methodology contained, however unconsciously, multiple serious design flaws biased against assisted dying: flaws which were brought to the attention of the AMA executive separately by two survey design experts. The executive dismissed the criticisms, incoherently arguing that while the AMA’s reviews are “fully-informed decisions based on well-researched, comprehensive information,” the survey was “not formal ‘research’ as such” and merely a “means to engage our members.”
The AMA relied on selected statistics from the survey to publicly explain the outcome of its review. It also provided its own members a private, detailed report of the review, of which more than half was a comprehensive statistical analysis of the survey.
The ‘Survey Limitations’ section of the report mentioned several minor issues, but not the significant biases brought to the attention of the executive by experts.
Yet supportive doctor responses
Despite these significant biases against assisted dying, the survey found:
68% of doctors said that even with optimal care, complete relief of suffering is not always possible.
60% of doctors said that if lawful, euthanasia should be provided by doctors, and more than half of them (total 32%) said that they would indeed practice it.
52% of doctors said that euthanasia can form a legitimate part of medical care.
50% of doctors expressly disagreed with the AMA’s statement that “doctors should not provide euthanasia under any circumstances.”
38% of doctors expressly disagreed with the AMA’s policy opposed to assisted dying (only half expressly agreed), and 35% of doctors said that euthanasia should be lawful.
Some doctors oppose legalisation, not euthanasia itself
In relation to the last point, other scholarly research has found that an additional 25% of Australian doctors are opposed to law reform not because they are opposed to assisted dying itself, but because they would rather practice it in private without regulatory ‘interference.’ This confirms that more than half of Australian doctors believe assisted dying can be a legitimate and practical part of medical care.
AMA not representative of Australian doctors
Only AMA members were invited and permitted to participate in the survey, and more than 70% of Australian doctors are not AMA members, despite the AMA expressly advancing itself as representing all Australian doctors. Non-members are likely to be more supportive of assisted dying — snubbing AMA membership due to the AMA’s ‘officially’ hostile stance.
Hostile tweets by President during review
During the review process, AMA President Dr Michael Gannon made repeated public statements hostile towards assisted dying, including a statement that doctor assisted dying would offend the Declaration of Geneva. The Declaration has nothing specific to say about assisted dying, and any general Declaration statements Dr Gannon relied upon would be equal arguments against abortion. Yet the AMA accepts abortion practice by doctors.
Indefensible conclusion by AMA Executive
Finally, in the face of ample evidence (despite the methodological biases) that at least half of the AMA’s own members favour doctor involvement in lawful assisted dying and deem it legitimate medical care, and 38% of its own members expressly disagreeing with its opposed policy, the AMA executive decided to maintain ‘official’ organisational opposition in the revised PS.
The PS, which was previously named broadly as about ‘end of life care’, is now exclusively named as about ‘euthanasia and physician assisted suicide,’ even though it continues its broad coverage. This suggests that, however unconsciously, the executive’s attitudes against assisted dying have become more entrenched.
The PS continues to unequivocally state as before that “The AMA believes that doctors should not be involved in interventions that have as their primary intention the ending of a person’s life.” In announcing the conclusions of its review the AMA has promoted this statement widely and as though it applies to all Australian doctors, most of whom are not AMA members.
Neither AMA 'policy' nor its Code of Ethics is binding
Despite the confidence and certainty of the statement, the AMA advises that neither Australian doctors in general nor even its own members are bound by its PSs. Thus, statements in AMA PSs are more ‘suggestions’ or ‘thought bubbles’ rather than authoritative statements.
More recently, the AMA’s Code of Ethics has been updated, yet remains entirely silent on doctor-assisted dying, in curious contradiction of the ‘certainty’ of its PS. The Code of Ethics is not binding on doctors (even AMA members), either.
Incoherent demands for policy consultation
The AMA executive continues to demand deep involvement in the development of a legal framework for assisted dying (despite saying that doctors should not be involved in the practice), yet it has developed no specific frameworks for three other related, already-lawful medical practices: refusal of life-preserving medical treatment, continuous deep sedation until death, and the voluntary refusal of food and fluids.
These discrepancies collectively raise the question as to whether the AMA’s ‘official’ opposition to assisted dying law reform is political rather than medical.
Conclusison
The evidence is clear that the only “justifiable” position the AMA executive could have taken was to declare the AMA neutral towards lawful assisted dying — a matter of individual conscience for its member doctors.
Australian doctors may well question the AMA executive as to how such a flawed process arrived at the outcome it did, and a collection of questions are posed for the AMA to answer. Sixteen questions are posed below.
Why does the AMA, through its Tasmanian representative, think it appropriate to state on national television that dying patients in extremis and without relief can suicide by themselves, even if the AMA doesn’t “encourage” it?
Why did the AMA repeatedly delete corrections to its negative MJA misinformation about assisted dying practice in Belgium?
Why did the AMA decide to review its “policy on euthanasia and physician assisted suicide” when it didn’t specifically have one? It had a policy on the role of doctors in end of life care.
Why did the AMA review comprehensively ignore the substantial secondary data that already exists about the attitudes and practices of doctors and patients in end of life decisions?
Why did the AMA not proactively obtain professional advice and assistance with the design and conduct of its doctor survey, and prefer to use such an amateurish one?
If the AMA really represents all Australian doctors, why did it expressly exclude more than two thirds of them from its survey?
Why did the AMA persistently use inappropriate language and inadequate definitions about assisted dying?
Why did the AMA not make any serious attempt to understand patient perspectives beyond superficial statements that ‘opinions are divided’?
Why did the AMA not report the multiple significant biases in its survey, which it knew about, in the ‘limitations’ section of its final report?
Why did the AMA President consider it appropriate to make multiple statements hostile towards assisted dying while the review was underway?
Why did the AMA executive decide to continue to demand doctors not participate in assisted dying, when more than half of its own members said it could be appropriate clinical practice provided by doctors, nearly four in ten expressly disagreed with the policy, and a third said they’d participate if assisted dying were legalised?
Why does the AMA consider it appropriate to make repeated categorical, public statements that doctors should not be involved in assisted dying, when its Position Statement is not binding on its own members, let alone all Australian doctors?[1]
How can the AMA justify the incoherence of having an expressly opposed stance to assisted dying in its revised Position Statement while it remains totally silent on the matter in its Code of Ethics, revised at the same time?
How can the AMA legitimately demand to be centrally involved in developing an assisted dying framework — in which it says doctors should not be involved — for law reform, when it has no frameworks at all for the similar contexts of refusal of life-preserving medical treatment, continuous deep sedation until death, and the voluntary refusal of food and fluids (all currently lawful and practiced)? When will it develop and publish those?
Why does the AMA continue to present itself to the media and the public as representing all Australian doctors, when more than two thirds of them are not members?
Will the AMA include a formal analysis and critique of this deeply flawed policy review as part of its modernisation efforts in order to rebuild its brand value and stem the falling tide of its membership? That is, is the AMA prepared to learn from its mistakes?
[1] The AMA’s Code of Ethics is not binding even on its own members, either. So when the Code states “don’t engage in sexual, exploitative or other inappropriate relationships with your patients,” that’s merely a ‘suggestion’ or ‘recommendation’ rather than an ‘obligation’ as a member of the AMA.
“#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
Her just-published IAHPC ‘Concept Note’ railing against assisted dying,1 and summarised on the European Association of Palliative Care’s (EAPC) website,2confirms and amplifies precisely the point I made.
Now you’d think that an organisation with a name like ‘International Association for Hospice and Palliative Care’ would be a neutral organisation representing the world profession irrespective of the faith or personal spiritual beliefs of its members.
But you’d be quite wrong.
Nothing but Catholic doctrine
The IAHPC's musings extensively cite several Popes as the authorities on the subject of — and exclusively against — assisted dying. They expressly use the term "Table of authorities," which includes Popes. And who else?
Precisely nobody: no other faith, and no impartial scientific research, is cited. Just Popes.
She also writes:
“IAHPC wishes to encourage our partners to express clear support for faith based teachings on palliative care.”
“It is important to clarify this misinformation [about ‘stealth euthanasia’] with the authoritative teachings of the Church.”
“Hospice has always been faith based.” [As if ‘the way it’s always been’ is a sound argument for ‘the way it always should be.’ Perhaps we shouldn’t have moved from serfdom to democracy?]
“The Catholic Church began the medieval hospice movement, and can lead the modern palliative care movement.” [They curiously neglect to mention that the palliative care (not hospice) movement rose from Anglican roots in the UK, helpfully confirming that this broadcast is primarily about promoting Catholic religion, not palliative care.]
Shameless self-promotion
But Dr Pettus and the IAHPC’s Concept Note don’t stop there.
“The Word [sic] Day of the Sick (WDS) is a good opportunity to support faith based healthcare organizations.”
“Contact your parish to see if you can hold a small event…”
“Contact your local Catholic health care provider director to find out about…”
“Make an announcement at your local church…”
Gosh, I must have been mistaken. I thought World Day of the Sick was about… the sick!?
But Dr Pettus and the IAHPC commandeer it to shamelessly further the Catholic religious agenda amongst palliative care service providers.
An unexamined conflict of interest
It's deeply disturbing that someone holding the position of “Advocacy and Human Rights Officer” considers the beliefs and values only of the service provider (who she represents) in promoting the world day about sick people (who her organisation serves).
Palliative care organisations repeatedly state that they aim to deliver patient-centred care. But the world palliative care peak body's self-adoration exposes the worst of them: taking the opportunity of a day supposedly for the values and needs of sick patients, and using it to glorify their own particular (Catholic) religious tenets which are to be lauded over those of the patients they serve.
Most of the world is not Catholic, and in Australia at least, most Catholics disagree with Vatican doctrine on assisted dying.
How astonishing then to dictate that Catholic doctrine must prevail over everyone, including Protestants, Hindus, Buddhists, Jews, Muslims, agnostics, atheists and others. Dr Pettus and the IAHPC comprehensively fail to demonstrate any awareness or reflection of potential conflicts of interest in serving people of different faiths and beliefs.
Incomprehensible arrogance
There is little issue with the Catholic Church directing its own willing adherents as to how they might end their days.
But for one religious institution to seek to impose its views on everyone worldwide is incomprehensibly arrogant. I guess it's no surprise then that a Catholic Bishop recently admitted — at a Royal Commission inquiry into the extensive, ongoing and horrific abuse of children under the Church's pastoral care — that the Catholic Church is a "law unto itself".
It would be helpful if the Holy See reflected on the principle: is it legitimate for another faith to force its own views on the Vatican or on Catholic patients?
It would also be helpful if the International Association of Hopsice and Palliative Care reflected on respecting and serving the wider community rather than behaving like a subsidiary of the Holy See.
Conclusion
The IAHPC has provided its own unequivocal proof that it is religious conservatism behind organised opposition to assisted dying, with the Catholic Church at the front of the pack.
You’ll understand why I tweeted in response to Dr Pettus:
“.@kpettus @EAPCOnlus Thanks for confirming @Pontifex arrogance. Not once did you mention PATIENT’S PoV. All about YOU.” — Neil Francis
- - -
And furthermore
Parading ignorance
The IAHPC refers repeatedly to the treatment of ‘pain’ in its stand against assisted dying law reform. But pain is not amongst the leading reasons for assisted dying (it is a much less common reason). Key reasons are the inability to participate in any of life’s enjoyable activities, loss of independence and loss of dignity.
I guess the curious focus on ‘pain’ is understandable though, because the Vatican is very fond of the doctrine of double effect (DDE) — which the IAHPC specifically notes in Catholic Catechism 2279 although not by its DDE name, but rather bizarrely as “a special form of disinterested charity.”
The DDE posits that it’s OK for a doctor to administer high doses of analgesics to treat pain, even if an unintended consequence is to hasten the patient’s death. The Catholic Church treats this doctrine as uncontroversial, even though it remains controversial amongst other ethicists and philosophers: the principle says “it’s quite OK for a doctor to kill her patient, as long as she doesn’t really mean to.”
I would commend Dr Pettus and the IAHPC to do some proper research and understand the subject area more competently before pontificating (yes, intended meaning) further.
The smokescreen argument
The IAHPC also states that:
“No country or state should consider the legalization of euthanasia or PAS until it ensures universal access to palliative care services.”
That’s purely a smokescreen argument for two reasons. Firstly, the Concept Note also argues that assisted dying:
“both violate[s] the bond of trust within the profession of medicine, and undermine[s] the integrity of the profession and the dedication to safeguard human life.”
Setting aside the empirical falsehood of the statement, it furnishes the IAHPC a 'get-out-of-jail-free' card if and when palliative care becomes ‘universally’ available: it’s utterly irrelevant if that goal is reached because there’s a more fundamental objection behind it.
Secondly, it's an established fact that palliative care can’t always help, even when the best services are available. ‘Universal’ access won’t fix all the problems.
All these faux arguments are typical and common from religious opponents of assisted dying.
Blog by Neil FrancisPosted on Thursday 9th February 2017 at 9:53pm
You only have to look to understand who is campaigning against your right to choose an assisted death in the face of intolerable and unrelievable suffering.
A case in point is a massive advertisement published in both of Melbourne’s daily newspapers: News Corp’s The Herald Sun (right-wing) and Fairfax Media’s The Age (left-wing). The ad was published in 2008 when Victorian MLC Colleen Hartland introduced the Medical Treatment (Physician Assisted Dying) Bill into the State legislature.
The Catholic Archbishop of Melbourne, Denis Hart, also sent the advertisement as a letter to all members of the Victorian Parliament.1
So, who are the advertisement’s signatories? I’ve listed them all in Table 1.
Table 1: Signatories to the 2008 Victorian anti-assisted-dying advertisement
Rt Rev. Graham Bradbeer
Moderator, Presbyterian Church of Victoria
The Rev. Fr Graeme A. Michell, FSSM
Parish Priest, Anglican Catholic Parish of St Mary the Virgin, Melbourne
Rev. Ross Carter
Uniting Church in Australia
Pastor Graham Nelson
Senior Pastor, Life Ministry Centre
Rev. Dr Max Champion
National Chair of the Assembly of Confessing Congregations within the Uniting Church in Australia
Rev. David Palmer
Convenor Church and Nation Committee, Presbyterian Church of Victoria
Pastor Mark Conner
Senior Minister of CityLife Church
Rev. Greg Pietsch
President, Victorian District, Lutheran Church of Australia
Dr Denise Cooper-Clarke
Adjunct Lecturer, Ridley Melbourne Mission and Ministry College
Rabbi Dr Shimon Cowen
Director Institute for Judaism and Civilization
Very Rev. Dr Michael Protopopov
Dean - Russian Orthodox Church in Australia
Rev. Megan Curlis-Gibson
St Hilary’s Anglican Church, Kew
Marcia Riordan
Respect Life Office, Catholic Archdiocese of Melbourne
Archbishop Dr Philip Freier
Anglican Church of Melbourne
Metropolitan Archbishop Paul Saliba
Primate of Antiochian Orthodox Archdiocese of Australia, New Zealand & the Philippines
Imam Riad Galil
West Heidelburg Mosque
Member of the Victorian Board of Imams
Bishop Peter Stasiuk CSSR DD
Eparchy of Saints Peter and Paul of Melbourne, for Ukrainian Catholics in Australia and New Zealand
Rev. Father James Grant SSC
Chaplains Without Borders,
Melbourne Anglican Diocese
Dale Stephenson
Senior Pastor Crossway Baptist Church
Assoc. Professor Afif Hadj MB BS (Melb) FRACS
Director of Surgery, Director of Medical Training, Maroondah Hospital (A Monash University Teaching Hospital)
Pastor Peter Stevens
Victorian State Officer
Festival of Light Australia
Archbishop Denis Hart
Catholic Archdiocese of Melbourne
Dr Nicholas Tonti-Filippini
Associate Dean, JPII Institute for Marriage and Family Melbourne
Rev. Fr Geoff Harvey
Priest of the Good Shepherd Antiochian Orthodox Mission Parish, based at Monash University
Rob Ward
Victorian State Director Australian Christian Lobby
Assoc. Professor Rosalie Hudson
Aged Care & Palliative Care consultant/educator
Jim Zubic
President of Orthodox Chaplaincy Association
Peter McHugh
Senior Pastor Christian City Church, Whitehorse
Persons in blue: Career is religion
Almost all of them are religious by career
To save you a lot of time assessing who these people are, I’ve coloured in blue all the folks whose job it is to espouse religion — at least, their own hierarchy’s view of it.
That’s 27 of the 29 signatories who by career are intensely immersed in their own religious perspective of the world; established and promoted through institutional doctrine.
But what about the other two?
What about the other two signatories, Assoc. Prof. Afif Hadi and Assoc. Prof. Rosalie Hudson (in yellow)?
Notice that Prof. Afif Hadi’s entry lists only his surgery profession. Highly relevant, but not mentioned, is that he was President (previously Vice Chairman) of the Australian and New Zealand Board of Trustees, Antiochian Orthodox Archdiocese of Australia and New Zealand. As head of the Board of the Archdiocese, his religious signature is intimately entwined with another: Metropolitan Archbishop Paul Saliba, the Primate of the Antiochian Orthodox Archdiocese.
Assoc. Prof. Rosalie Hudson’s listing too, mentions only seemingly secular links. What is omitted is that she is or was Chair of the University of Divinity (a multi-faith religious institution) Human Research Ethics Committee, Secretary of the Uniting Church’s committee on bioethics, a member of the Interfaith Committee, and an Academic Associate at Charles Sturt University’s School of Theology.
Thus, both Prof. Hadi and Assoc. Prof. Hudson are also deeply rooted in religious faith. The point is not to make any criticism of their faith or practice, but merely to observe the deeply religious connections to opposing assisted dying law reform. It’s worth mentioning that both Hadi and Hudson do valuable charity work.
So, all of them are deeply religious
A pertinent question to ask is: ‘What proportion of the signatories are neutral, scholarly researchers who have studied the empirical evidence from jurisdictions where assisted dying is already lawful?’ Answer: None of them. Enough said.
And what proportion of the signatories to this anti-assisted dying advertisement are very deeply invested in organised religion? The simple answer is as usual: 100%,all of them.
Disconnected from their flocks
Critically, these career-religious fail to reflect the views of their own flocks. We know from repeated polls, for example, that three out of four Australian Catholics, more than three out of four Uniting Church members, and four out of five Anglicans (Church of England) support assisted dying law reform.
This kind of clerical disconnect from the contemporary will of the people is one of the key reasons Australians are deserting religion in droves, as successive censuses show.
Conclusion
The evidence is irrefutable. Those who are actively organised to oppose your right to choose an assisted death are deeply religious, even when they use seemingly secular arguments (more on those later).
They are entitled to their opinions for themselves. But what right do they have to deny the vast majority of Australians, who do not agree with their views, the right to choose?
To phrase it in the personal, why does the Catholic Archbishop of Melbourrne, Denis Hart, think it appropriate to demand that Mr Geoff Drummond, a Buddhist, should have suffered against his will at the end of life for the Archbishop's version of faith, rather than Mr Drummond's own spiritual beliefs? Why does Rabbi Shimon Cowen think it appropriate to demand that Mr Alan Rosendorff, a fellow Jew, should have suffered against his will at the end of life for the Rabbi's version of faith, rather than Mr Rosendorff's own carefully-considered and deeply-held views? And why does Imam Riad Galil think it appropriate to demand that Mr Peter Short, not a Muslim, should have suffered against his will at the end of life for the Imam's beliefs, rather than his own?
Perhaps hubris remains alive and well amongst religious conservatives?
-----
Declaration: In fairness to those mentioned in this article, I openly declare that I am agnostic.
References
Bradbeer, G, Rt Rev., Carter, R, Rev., Champion, M, Rev. Dr, Conner, M, Pastor, Cooper-Clarke, D, Dr, Cowen, S, Rabbi Dr, Curlis-Gibson, M, Rev., Freier, P, Archbishop Dr, Galil, R, Imam, Grant SSC, J, Rev. Fr, Hadj, A, Assoc. Prof., Hart, D, Archbishop, Harvey, G, Rev. Fr, Hudson, R, Assoc. Prof., McHugh, P, Michell, GA, Rev. Fr, Nelson, G, Pastor, Palmer, D, Rev., Pietsch, G, Rev., Pietsch, M, Protopopov, M, Very Rev. Dr, Riordan, M, Saliba, P, Metropolitan Archbishop, Stasiuk, P, Bishop, Stephenson, D, Stevens, P, Pastor, Tonti-Filippini, N, Dr, Ward, R & Zubic, J 2008, Reject physician assisted dying - An open letter to Victorian MPs, Catholic Archdiocese of Melbourne, viewed 13 Jun 2008, http://www.cam.org.au/Euthanasia.aspx.
Blog by Neil FrancisPosted on Friday 2nd December 2016 at 5:34pm
The AMA announces an 'update' of its "euthanasia and physician assisted suicide" policy.
The Australian Medical Association (AMA) executive (policy group) recently concluded a major review of its official policy on assisted dying. The last major review was in 2007. Through a deeply flawed process the AMA executive continues to expressly disrespect the diversity of views amongst Australian doctors — a diversity confirmed by its own review — and hasn’t altered its opposition to assisted dying in any meaningful way.
Unrepresentative of Australian doctors
The AMA promotes itself as “leading Australia’s doctors,” yet more than two thirds of Australian doctors (70.5%) are not members. Its executive might like to think it’s leading, but most Australian doctors aren’t following. Claimed representation is particularly important when it comes to professional medical practice policies, because the AMA behaves as though its policies apply to all Australian doctors.
So who did the AMA consult in conducting its major review of policy on assisted dying? Only its own members. In other words, the AMA claims to represent all Australian doctors, but in reality consulted less than a third of them in the setting of its assisted dying policy. As AMA member Dr Rosemary Jones pointed out, some doctors eschew the AMA because of its opposed stance towards assisted dying. That creates a sampling bias in the AMA’s study… against assisted dying.
Further, the response rate to its survey of members was around 13%, meaning that only the most engaged AMA members (thus around 4% of all Australian doctors) offered a voice.
Biased survey
There are numerous flaws in the AMA’s survey. Here’s just one. In the preamble to the questionnaire, the AMA expressly told responding doctors (who, remember, are AMA members and probably don’t want to tick off their association) what its positions on certain end-of-life practices were. Then, in the first questions, it asked the doctor whether they agreed with the positions: strategies certain to result in substantial confirmation and acquiescence biases.
This just isn’t on. As a professional social and market researcher, I sent a detailed critique of the many problems with the survey to AMA President Dr Michael Gannon. I received a courteous but dismissive response from administration. A highly-respected Fellow of the Australian Market & Social Research Society sent a similar critique, also receiving a non-committal reply.
Survey results
While the AMA hasn’t published the survey results in detail yet, key headline statistics have been reported. What did the AMA discover on the basis of a methodology swayed against assisted dying?
Around four out of ten doctors believe that doctors should be involved in assisted dying cases, while around five out of ten thought they shouldn’t. One out of ten had no view either way.
If assisted dying were legalised, a majority said that doctors should be the ones to do this work.
That’s a clear message that a substantial proportion of doctors think assisted dying can not only be legitimate practice, but is the business of the medical profession — at least for those who wish to participate.
Executive’s ‘interpretation’
And what did the AMA executive make of these important insights after deliberating on them for months? Here are the AMA’s previous and ‘revised’ core policy statements:
Previous (2007) statement
‘Revised’ (2016) statement
“The AMA believes that medical practitioners should not be involved in interventions that have as their primary intention the ending of a person's life. This does not include the discontinuation of futile treatment.”
“The AMA believes that doctors should not be involved in interventions that have as their primary intention the ending of a person’s life. This does not include the discontinuation of treatments that are of no medical benefit to a dying patient.”
Despite the gratuitous change of a few words after a year of ‘research,’ the statement remains the same.
Doctors and the public have a right to ask of the AMA, “what part of the evidence that there is a genuine diversity of respectable views, did you miss?”
Failure to respect diversity
The executive might argue that it did listen. Here are its statements about diversity:
Previous (2007) statement
‘Revised’ (2016) statement
“The AMA recognises that there are divergent views regarding euthanasia and physician-assisted suicide.”
“The AMA recognises there are divergent views within the medical profession and the broader community in relation to euthanasia and physician assisted suicide.”
Despite another increase in wordiness, this statement too remains the same.
The AMA executive says it recognises that there are divergent views, but by continuing to insist that no doctor should be involved in assisted dying, it reveals that it doesn’t respect some views. How does it justify this hubris?
Failure to respect the patient
The revised policy also says in part:
“Doctors should … endeavour to uphold the patient’s values, preferences and goals of care.”
The sting in the policy tail is, given the AMA executive’s wholly opposed stance toward assisted dying, that the doctor should only uphold patient values, preferences and goals of care if the AMA executive approves of them (and assuming to do so is legal).
Was it a foregone conclusion?
The AMA executive’s continued opposition to assisted dying was unsurprising. The signals were clear. While the policy review was in play, AMA President Dr Michael Gannon made a series of tweets and media comments, all unsupportive of or directly opposed to assisted dying. Here’s a few.
In response to an article in The Australian “Catholic stance allows eased exit”, he tweeted a faux ‘competition’ between palliative care and assisted dying:
@amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian
He also tweeted in support of the ‘doctrine of double effect’, a controversial policy (which the AMA promotes as uncontroversial) that contends it’s quite OK for a doctor to hasten a patient’s death after all… provided they don’t really mean to: hardly a robust or verifiable standard.
@amapresident 24 Aug 2016: Doctors should be careful, must obey the law and understand their code of #ethics. Double effect is not #Euthanasia
In an article in The Australian on 15th September, Dr Gannon argued against assisted dying on the basis of it being ‘extremely complex.’ If complexity were a reason to oppose anything, the AMA would be opposed to the entire healthcare system: it’s incredibly complex. His argument collapses at the slightest inspection.
@amapresident 18 Sep 2016: Hippocratic medicine older than some of the world’s great religions, every political ideology, trend #ethics @medwma
Dr Gannon then invoked the Hippocratic Oath, which bans assisted dying. That’s cherry-picking at its best. Doctors do not take the Hippocratic Oath: it swears allegiance to ancient Greek gods, forbids women from entering the profession and outlaws surgery, amongst other things.
@amapresident 19 Sep 2016: Agree @DrSallyCockburn admire #euthanasia work done by @CMA_Docs. Equally careful, compassionate, intelligent approach from @TheBMA #ethics
He commends the British Medical Association’s “intelligent approach” against assisted dying: an approach I have comprehensively exposed as superficial and ill-informed fear-mongering, fiction, flip-flop and hubris.
@amapresident 1 Oct 2016: It is inevitable that if #Euthanasia laws are passed, they will over time be expanded to include children, mentally ill, vulnerable #ethic
Dr Gannon demonstrated ignorance of basic facts with this ‘slippery slope’ claim. In Oregon, which has the world’s oldest specific assisted dying framework (in effect since 1997), there have been no changes in who may qualify. He also ignores peer-reviewed research showing no ‘slippery slope’ for the supposed ‘vulnerable’. Canadian Professor Harvey Chochinov, Chair of his government’s expert panel which investigated legislative options for assisted dying, confirmed the evidential absence of the ‘slippery slope’ in a keynote address at Swinburne University in Melbourne last week.
@amapresident 11 Nov 2016: Doctors maintain this Trust with everyday care for patients, by upholding #DeclarationOfGeneva @medwma @juliamedew @Rania_Spooner #ethics
Dr Gannon also claimed that assisted dying would erode patient trust in doctors, at odds with the fact that people’s trust in doctors is high amongst OECD countries with assisted dying laws. Indeed, trust in doctors amongst Dutch, Belgian and Swiss citizens is significantly higher than Australians’ trust in our own doctors.
During the review period, Dr Gannon also repeatedly promoted the (medical) Declaration of Geneva (e.g. see previous tweet), which states that doctors must not participate in assisted dying. If the Declaration’s canonical opposition was indeed the authoritative stance on assisted dying, then it would be irrelevant for the AMA to conduct a review process of its policy.
Doctors and the public might ask a legitimate question: “Why did the AMA President think it appropriate to publicly and repeatedly indicate what review conclusion he favoured, while the review was in progress?”
Declining to correct misinformation
In September, the Medical Journal of Australia (MJA: a wholly-owned subsidiary of the AMA), published a news report containing significant misinformation that painted a hostile picture about assisted dying in Belgium. I published a critique of why the opinion was wrong, and commented on the online MJA article with a link to my correction. The MJA promptly deleted my comment.
AMA member Dr Rosemary Jones then put up the same objection which, by dint of her membership, they wouldn’t delete. The MJA then responded, but only to dig in its heels to defend the misinformation and reveal even more serious flaws in its arguments.
I wrote a further research-backed analysis of why its defensive arguments were even more wrong than the original and posted a note and link on the original MJA article page (Figure 1).
Figure 1: The second post on MJA inSight which was subsequently deleted.
Once again, my post has been deleted. The result of this is that erroneous information about Belgium remains published on the MJA website as though it is correct, while failing to mention or acknowledge that it has been soundly refuted.
It’s disappointing that the AMA and its President continue to make such uninformed remarks given that Dr Gannon claims to be a stickler for scientific evidence:
@amapresident 18 Aug 2016: Being a doctor is a huge privilege. Also carries responsibility to provide accurate scientific info, act ethically.
Spotlight on the AMA
Legitimate questions serve to shine a spotlight on the AMA. Firstly, given the circumstances, what was the likelihood of a real change to the AMA’s entrenched opposition toward doctor participation in assisted dying?
Secondly, given the AMA’s entrenched opposition, how can it expect its demands that it be consulted about any potential law reform to be treated seriously? If assisted dying is nothing to do with doctors, why is what doctors think relevant?
Utterly resistant to modernisation?
At its 2016 AGM, AMA member Dr Harry Hemley noted that the AMA largely represented its more hard-core, long-term older members and warned of the AMA’s increasing irrelevance and impotence (Figure 2). He moved an urgency motion to commission a review and report with “recommendations for a plan, vision and determination that will lead to re-invigorating and sustaining the AMA.”
Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform
The motion wasn’t in relation to an actual or particular reform: merely to investigate the potential for reform and to provide recommendations for consideration. We can only hope that the AMA will drag itself into the 21st century at some stage.
Conclusion
The AMA is deeply out of touch with Australians on the issue of assisted dying. It represents fewer than a third of Australian doctors and has failed to respect the very range of perspectives it obtained by consulting its members. It further strains its credibility by insisting that doctors mustn’t be involved in assisted dying, yet demanding to be consulted on any law reform to permit it.
If the AMA is to become relevant to contemporary society it must move on from the ‘old boy’ approach to medicine and adopt a stance of neutrality toward assisted dying. Only neutrality demonstrates appropriate respect for the true range of views held in good conscience by Australian doctors.



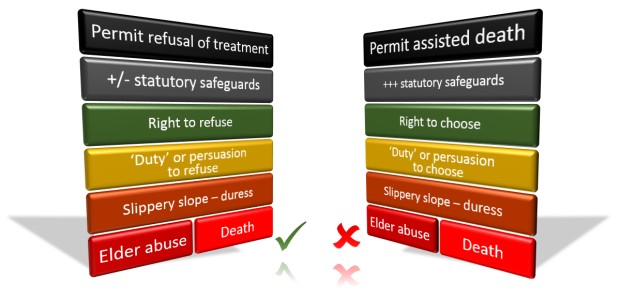 The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.


 Figure 1: Attitudes toward assisted dying by major religious denominations
Figure 1: Attitudes toward assisted dying by major religious denominations Figure 2: Attitudes toward assisted dying by frequency of attending religious services
Figure 2: Attitudes toward assisted dying by frequency of attending religious services Figure 3: Frequency of attending religious services amongst those with a religious affiliation and who disagree with assisted dying
Figure 3: Frequency of attending religious services amongst those with a religious affiliation and who disagree with assisted dying Figure 4: Attitudes by religious service attendance plus denomination affiliation (“Regulars”)
Figure 4: Attitudes by religious service attendance plus denomination affiliation (“Regulars”)
 Figure 1: Assisted dying in Benelux and North America as a percentage of all deaths
Figure 1: Assisted dying in Benelux and North America as a percentage of all deaths
 Infographic summary of 'AMA uncovered'
Infographic summary of 'AMA uncovered'
 “#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
“#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
 Figure 1: The second post on
Figure 1: The second post on  Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform
Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform