The F filesPosted on Tuesday 9th April 2019 at 7:15am
An article in 'Anasthesia' did NOT find high rates of regaining consciousness in contemporary VAD practice.
A recent article by Sinmyee et al, "Legal and ethical implications of defining an optimum means of achieving unconsciousness in assisted dying", published in the journal Anasthesia1 was an attempt to identify a professional standard for inducing and maintaining unconsciousness prior to voluntary assisted dying (VAD) death, a laudable aim.
However, the authors’ underlying premise of contemporary VAD practice failing to reliably maintain unconsciousness — potentially leading to 'inhumane deaths' — is not established by their cited sources. They cite exactly three sources to establish their claim: their citations 31, 32 and 33.
Citation 31 — Iserson et al 1992
This is a qualitative article by Ken Iserson and colleagues.2 Published in 1992, it outlines a single case of assisted suicide, forming the backdrop for several Californian ethics committees to comment.
Not only was this a single case rather tha a sample of dozens or hundreds of cases, but assisted dying was illegal right across the USA in 1992 and earlier. Therefore, the article is wholly uninformative to contemporary practice under assisted dying laws.
Citation 32 — Groenewoud et al 2000
This is a study by Johanna Groenewoud and colleagues.3 Published in 2000, it analyses Dutch data collected between 1990 to 1996 — long before the Netherlands’ 2001 euthanasia Act, which came into effect in 2002.
In 1997 the Dutch medical association (KNMG) formed the Support and Consultation on Euthanasia in Amsterdam (SCEA) network to assist doctors implement the practice more reliably. The successful program was made national (…in the Netherlands, SCEN) in 1999, with a four-year implementation resulting in strong consultation and positive outcomes.4
In addition, the KNMG and Dutch pharmacy association (KNMP) have improved their guidelines for euthanasia practice since 1996: in 1998, 2007 and most recently in 2012.5 Independent studies show that use of opioids (inappropriate method) was high in the Netherlands in 1995-96,6 but replaced entirely with (appropriate) barbiturates and neuromuscular relaxants in reported VAD cases in 2010.7
The most recent published report of the Dutch Euthanasia Commission, which assesses every reported case of VAD, did not note any failures of the VAD procedures.8
Citation 33 — Lalmohamed & Horikx 2010
This is a study by Arief Lalmohamed and Annamieke Horikx, published in 2010, of doctor responses to a survey the KNMP conducted between 2007 and 2009.9 The study reported on issues with the storage, preparation and administration of VAD drugs. It noted that the recommended dose of Thiopental was increased from 1500mg to 2000mg so that patient-dependent dosages need not be calculated.
The study noted one negative experience for some patients: pain on injection of Thiopental. Recommendations were made for preparation and administration of the drug to avoid this problem. No other negative patient outcomes were reported.
The upshot
Thus, of the three sources the authors employed to make the case of a significant and systematic problem in the conduct of contemporary VAD cases, none did so: the first was a single case outside the law in the early 1990s, the second a study from the early to mid 1990s from whence contemporary practice has greatly improved, and the third a 2010 pharmacological investigation that found some patients experiencing pain on injection and recommending improvements to avoid it. Nevertheless, Sinmyee et al concluded that:
“For all these forms of assisted dying, there appears to be a relatively high incidence of vomiting (up to 10%), prolongation of death (up to 7 days), and reawakening from coma (up to 4%), constituting failure of unconsciousness.”
These assertions are highly misleading in regard to contemporary VAD practice.
The most recent Oregon Death With Dignity Act annual report, covering all cases from 1997 to early 2019 reports that just eight of 1,467 deaths where lethal medication was consumed, resulted in the patient regaining consciousness.10 That’s an efficacy rate of 99.5%, a high standard for a medical procedure.
There have been no cases of regaining consciousness in Washington state under their Death With Dignity Act.11
In comparison, regaining consciousness under professional surgical anaesthesia is a problem12 with an incidence rate of around 0.13% in the USA13 though the rate appears to be much lower in the UK.14 Even over-the-counter analgesics like paracetamol, ibuprofen and aspirin have significant adverse effects rates of 14.5%, 13.7% and 18.7% (respectively).15
From unsubstantiated to polemical
While Sinmyee and colleagues were attempting, via their article in Anasthesia, to argue the case for improved VAD practice, it was inevitable that ginger groups opposing the legalisation of VAD would commandeer cherry-picked extracts from the article to further their cause, painting a picture of disaster and mayhem.
Sure enough, the Catholic-backed Euthanasia Prevention Coalition’s Alex Schadenberg ran with it, cherry picking the “190 times higher” rate the authors claim for “failure of unconsciousness” using their invalid citations. Schadenberg conspiratorially concluded that “the laws are designed to cover-up [sic] problems with the law”.16
Also, predictably, Catholic-backed HOPE’s Branka van der Linden followed suit, plucking quotes like “…failure rates of assisted dying by these other methods seems extraordinarily high” without similar context.17
It’s disappointing that the original article with its misleading statistics based on figures plucked from a single historical article and in the absence of considering significant intervening improvements, passed peer review. Its misinformation led to more nonsense being energetically pedalled by anti-VAD campaigners.
References
Sinmyee, S, Pandit, VJ, Pascual, JM, Dahan, A, Heidegger, T, Kreienbühl, G, Lubarsky, DA & Pandit, JJ 2019, 'Legal and ethical implications of defining an optimum means of achieving unconsciousness in assisted dying', Anaesthesia, 74(5), pp. 630-637.
Iserson, KV, Rasinski Gregory, D, Christensen, K & Ofstein, MR 1992, 'Willful death and painful decisions: A failed assisted suicide', Cambridge Quarterly of Healthcare Ethics, 1(2), pp. 147-158.
Groenewoud, JH, van der Heide, A, Onwuteaka-Philipsen, B, Willems, DL, van der Maas, PJ & van der Wal, G 2000, 'Clinical problems with the performance of euthanasia and physician-assisted suicide in the Netherlands', New England Journal of Medicine, 342(8), pp. 551-556.
Jansen-Van Der Weide, MC, Onwuteaka-Philipsen, BD & Van Der Wal, G 2004, 'Implementation of the project 'Support and Consultation on Euthanasia in the Netherlands' (SCEN)', Health Policy, 69(3), pp. 365-373.
KNMG/KNMP 2012, Guidelines for the practice of euthanasia and physician-assisted suicide, Utrecht, pp. 56.
van der Maas, PJ, van der Wal, G, Haverkate, I, de Graaff, CL, Kester, JG, Onwuteaka-Philipsen, BD, van der Heide, A, Bosma, JM & Willems, DL 1996, 'Euthanasia, physician-assisted suicide, and other medical practices involving the end of life in the Netherlands, 1990-1995', N Engl J Med, 335(22), pp. 1699-705.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, 380(9845), pp. 908-915.
Lalmohamed, A & Horikx, A 2010, '[Experience with euthanasia since 2007: Analysis of problems with execution] Ervaringen met euthanastica sinds 2007: Onderzoek naar problemen in de uitvoering', Ned Tijdschr Geneeskd, 154(A1983), pp. 1-6.
Oregon Health Authority 2019, Oregon Death With Dignity Act: 2018 data summary, Department of Human Services, Portland, pp. 16.
Washington State Department of Health 2018, Washington State Department of Health 2017 Death with Dignity Act Report, Olympia, WA, pp. 15.
Cook, TM, Andrade, J, Bogod, DG, Hitchman, JM, Jonker, WR, Lucas, N, Mackay, JH, Nimmo, AF, O'Connor, K, O'Sullivan, EP, Paul, RG, Palmer, JH, Plaat, F, Radcliffe, JJ, Sury, MR, Torevell, HE, Wang, M, Hainsworth, J, Pandit, JJ, Royal College of, A, the Association of Anaesthetists of Great, B & Ireland 2014, 'The 5th National Audit Project (NAP5) on accidental awareness during general anaesthesia: patient experiences, human factors, sedation, consent and medicolegal issues', Anaesthesia, 69(10), pp. 1102-16.
Sebel, PS, Bowdle, TA, Ghoneim, MM, Rampil, IJ, Padilla, RE, Gan, TJ & Domino, KB 2004, 'The incidence of awareness during anesthesia: A multicenter United States study', Anesthesia & Analgesia, 99(3), pp. 833-839.
Thomas, G & Cook, TM 2016, 'The United Kingdom National Audit Projects: a narrative review', Southern African Journal of Anaesthesia and Analgesia, 22(2), pp. 38-45.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
The F filesPosted on Saturday 18th November 2017 at 11:27pm
Jones, Paton and Kheriaty's articles demonstrate poor science and multiple, egregious instances of bias.
In 2015, Dr David Jones and Prof. David Paton published an article titled “How does legalization of physician-assisted suicide affect rates of suicide?” in the Southern Medical Journal. The article purported to establish suicide contagion from Oregon and Washington Death With Dignity Act (DWDA) deaths to “total suicides.” It also purported to establish no decrease in general suicide rates, which Jones & Paton argued should occur by substitution of assisted death for some general suicides. (Notice how these two ‘expected’ results — an anticipated rise and an anticipated fall in suicide rates — are at odds in principle.)
In my thorough and empirically-backed response, I expose the disgraceful playbook of these authors as they shambolically commit no fewer than ten deadly sins against science in the pursuit of their opposition to lawful assisted dying.
In 2015, Dr David Jones & Prof. David Paton published an article in the Southern Medical Journal titled “How does legalization of physician-assisted suicide affect rates of suicide?” This study examines the article, as well as an enthusiastic editorial of it by Dr Aaron Kheriaty in the same journal issue, both of which portray “suicide contagion” from Oregon and Washington’s death with dignity acts (DWDA).
However, while contagion from general suicides is a well-established phenomenon, there are multiple sound reasons to reject contagion theory in relation to assisted deaths, including:
Most healthcare professionals readily acknowledge key differences in the characteristics of assisted deaths: for example, a fully informed, tested and rational decision with shared decision-making.
Those using Oregon and Washington’s DWDAs are, by qualifying for it, already actively dying. Thus, they are choosing between two ways of dying rather than between living and dying.
Most of those using the DWDA discuss it with their families (expected, peaceful death), whereas most general suicides occur in isolation and without discussion (unexpected, often violent death).
Multiple studies show that while families of general suicide experience complicated bereavement, families of assisted dying cope at least as well as, and in some cases better than, the general population or those who considered but did not pursue assisted death.
Even if “suicide contagion from assisted dying” theory were sound, direct evidence from official government sources shows that the number of potential suicides in Oregon in 2014 would have been fewer than 2 in 855 cases: undetectable by general modelling methods.
Jones & Paton’s article title conveys an air of skilled and scientific neutrality. However, close examination of the article, and Kheriaty’s editorialisation of it, reveals least ten serious flaws or ‘scientific sins.’
The authors demonstrated little understanding of the complex issues surrounding suicide, willingness to unjustifiably equate assisted dying with general suicide, contentment with failing to search for, consider or include contrary evidence including from sources they cite to argue their case, unreasonable trust in a model that couldn’t hope to legitimately resolve their premises, satisfaction with executing their model amateurishly, a disposition to overstate confidence of causation in the absence of meaningful statistical correlations, and an inclination for emphasising results in accordance with their theories while de-emphasising or ignoring others.
Any of these flaws was serious enough to invalidate Jones & Paton’s article and Kheriaty’s conclusions of it, yet there is not one deadly flaw: there are at least ten.
Their claim of a supposed 6.3% suicide contagion rate from assisted dying in Oregon and Washington is a conceptual and mathematical farce.
The Southern Medical Journal is a peer-reviewed journal. However, it is difficult to reconcile the rigorous standards and sound reputation that peer review is intended to maintain, with the numerous, egregious flaws in this study and its dissemination.
Rather than inform the ongoing conversation about lawful assisted dying, the Jones & Paton and Kheriaty articles misinform and inflame it.
Given the numerous egregious flaws, both articles ought to be retracted.
The F filesPosted on Friday 14th April 2017 at 10:47pm
Professor Margaret Somerville makes an indefensible 'suicide contagion' claim.
Catholic ethicist Professor Margaret Somerville claims that every assisted suicide jurisdiction shows 'contagion' to the general suicide rate. The empirical evidence contradicts her claim.
Professor Margaret Somerville, currently Professor of Ethics in the School of Medicine at the Catholic University of Notre Dame Australia,[1] has enjoyed ongoing publication of her opinions, with few challenges published to date.
Back in 2007, Somerville, then a Professor of Ethics at McGill University in Montreal, Canada, appeared as an expert witness in an Iowa District Court case. The court comprehensively rejected her testimony, determining that she:
“…specifically eschews empirical research and methods of logical reasoning in favour of ‘moral intuition.’ She has no training in empirical research…”
Professor Somerville, I argue, has again fallen short on empirical research and logical reasoning. To illustrate, I will analyse her claim, published in an opinion piece in ABC Religion and Ethics that:
“…the general suicide rate has increased in every jurisdiction that has legalized assisted suicide.”
While her claim may be her own personal opinion, she has presented it expressly stating that she is a Professor of Ethics at her current university of employment, lending the claim perceived authority.
This report demonstrates how her claim and her defence of it are contradicted by multiple sources of empirical government and other primary research evidence. It also demonstrates that she failed to engage appropriate scholarly standards that require the active search for, acquisition and analysis of all reasonably available relevant data in an attempt to answer a particular question.
In making her claim, Prof. Somerville:
Cites ‘supportive’ data from lawful jurisdictions while overlooking other data, sometimes even in the same data set, that are inconsistent with her claim;
Cites as supporting evidence an econometric modelling study that did not find a statistically-significant relationship between assisted dying law and the general (non-assisted) suicide rate;
Fails to consider data from all jurisdictions with assisted suicide laws while making a claim about them all — overlooking Switzerland, whose empirical data is clearly at odds with her claim;
Repeatedly cites non-academic anti-euthanasia lobbyist Mr Alex Schadenberg (who also cites her) as a source of evidence for her claim and who in turn quotes a television source and another lobbyist’s opinion to underpin his own beliefs about ‘suicide contagion’; and
Conflates voluntary euthanasia (physician-administration) with assisted suicide (patient self-administration) such that her argument, at least in the context of Belgium and the Netherlands, is substantially about the novel concept of ‘euthanasia contagion’ rather than the more familiar ‘suicide contagion’ expression she uses.
These findings are consistent with the Iowa court’s ruling that Prof. Somerville sometimes relies on ‘moral intuition’ rather than sound empirical research and logical reasoning.
My report also draws a number of connections between those advancing misinformation on assisted dying ‘suicide contagion,’ and Catholic identity. Catholic identity is not a reason to reject arguments, but it does help identify the source of a majority of ‘suicide contagion’ misinformation.
Finally, I argue that the appropriate course of action for Prof. Somerville is to retract her ‘suicide contagion in every jurisdiction’ claim.
[1] Not to be confused with another Professor Margaret Somerville, who is Director of the Centre for Educational Research at Western Sydney University.
Blog by Neil FrancisPosted on Sunday 19th March 2017 at 11:37pm
Oregon (left) and Washington legalised assisted dying by ballot in 1997 and 2008 respectively. Photos: Oregon Department of Transportation; Cacophony.
A scientific study just published in the New England Journal of Medicine reveals that residents of both Oregon and Washington states, which legalised assisted dying in 1997 and 2008 respectively—as well as establishing formal advance directive programs—are far more likely to experience the kind of death they prefer, and with better access to palliative care, than is the average USA resident.1
It's well-established that most westerners would prefer to die peacefully at home rather than in a medicalised or other institutional setting. Yet it is recognised by doctors and families alike that there is a kind of medical ‘conveyer belt’ to acute care at the end of life that tends to shunt the dying individual through to ICU—a place where more and more burdensome medical interventions are administered with less and less likelihood that they’ll actually provide any benefit. These kinds of deaths, with vigorous and invasive procedures performed on a frail person approaching a natural death, can lead to longer and more complex bereavement recovery for surviving loved ones.
It’s also claimed by opponents of assisted dying law reform that assisted dying is a ‘competitor’ of palliative and hospice care, and that legalisation of assisted dying would result in the deterioration or at least stunting of palliative care services.
This latest study, including longitudinal data, provides further evidence that such claims are not only false, but that the legalisation of assisted dying improves the focus on all end of life decision making, whatever those decisions are.
Avoiding burdensome and questionable invasive care
Figure 1: ICU was used in the last 30 days of life Percent of fee-for-service Medicare service beneficiary patients
Figure 1 shows that the ‘shunting’ of dying patients to ICU in the last 30 days of life is significantly lower in Oregon, which legalised assisted dying in 1997. Oregon also established a statutory comprehensive advance care directive (Physician Orders for Life Sustaining Treatment, or “POLST”) program earlier than other states, in 1993. Washington, which piloted a POLST program in 2000 and formally endorsed it in 2005 — and legalised assisted dying by ballot in 2008 — was already trending down from the national average (close to it in 2000), as public discussion of end of life decisions ratcheted up in the lead-up to reform. Since the POLST endorsement and ballot reform, Washington has continued to trend well below the national average.
Facilitating a non-institutionalised death
Figure 2: Patient was discharged from hospital in the last 30 days of life
Figure 2 shows that both Oregon and Washington have continued to trend above the national average for facilitating patient wishes to die at home after a stay in acute care in the last 30 days of life.
Hospice care received at home
Figure 3: Dying patient received hospice care at home
Figure 3 shows that by 2000, Oregon was already providing home hospice services at 2.1 times the national average, but that as the national average plateaued from 2005, the rate in Oregon continued to rise significantly, reaching 2.5 times the national average in 2013. To qualify for an assisted death, Oregon and Washington residents must be certifed by their doctor as expected to die within six months—which qualifies the patient for free hospice care.
Washington was close to the national average on the delivery of home hospice care prior to assisted dying law reform, beginning to deviate as conversations were held about permitting assisted dying and its POLST program was endorsed in 2005, increasing to 1.8 times the national average in 2013.
Death preferred at home
Figure 4: The individual died at home
Figure 4 shows that both Oregon and Washington states continue to facilitate a private home-based death, according to patient and family wishes, at a rate considerably higher than the national average.
Conclusion
The results of this USA study mirror the kinds of findings from Dutch and Belgian research, which I have previously published,2 and another USA report from the Journal of Palliative Medicine which placed both Oregon and Washington amongst the top eight states for palliative care access in hospital settings.3 This study furthers these insights by showing that access to palliative care services in home settings is also significantly higher than the national average in Oregon and Washington.
Assisted dying opponents’ claims that legalising assisted dying would result in a deterioration or stunting of end of life decisions and in particular access to palliative care are contradicted by the data from lawful jurisdictions.
References
Tolle, SW & Teno, JM 2017, 'Lessons from Oregon in embracing complexity in end-of-life care', New England Journal of Medicine, 376(11), pp. 1078-1082.
Morrison, RS, Augustin, R, Souvanna, P & Meier, DE 2011, 'America's care of serious illness: A State-by-State report card on access to palliative care in our nation's hospitals', Journal of Palliative Medicine, 14(10), pp. 1094-1096.
Fact file by Neil FrancisPosted on Sunday 13th November 2016 at 1:47am
Assisted dying rates in Dutch-speaking cultures (orange bars) are much higher than elsewhere.
In this whitepaper, Benelux (Belgium, Netherlands and Luxembourg) primary empirical data on assisted dying is analysed — including with new and advanced approaches — to provide fresh insights into contemporary practices. Investigation reveals that the assisted dying rate in Dutch-speaking cultures appears to be uniquely higher than in other cultures irrespective of the permissiveness of the legislative framework, yet is still practiced conservatively.
Download a full copy of the Whitepaper here: PDF (648Kb).
Summary
This new compilation and unique analysis of primary research data from statutory authorities and the peer-reviewed literature provides fresh insights into assisted dying practice in Benelux, including:
Rates of assisted dying in the Netherlands and Belgium have followed an expected sigmoid curve, now beginning to level out.
Several factors have contributed to the higher increase in the Netherlands rate, including recovery from a suppression of cases immediately following statutory reform, a rise in cancer diagnoses, and an increase in granting of assisted dying through new visiting teams launched in 2012.
Both Netherlands and Belgium doctors demonstrate caution if not conservatism when assessing assisted dying requests.
Despite most assisted dying occurring in cases of cancer, fewer than one in ten cancer deaths in the Netherlands and one in twenty in Belgium is an assisted death.
Other conditions such as degenerative neurological, pulmonary and circulatory illnesses each account for a very small proportion of the increase in cases since legalisation in Benelux.
The assisted dying rate in dementia and other mental illness is very low despite controversy around—and a tiny rise in granting of—such cases.
The hypothesis that females or the elderly would be ‘vulnerable’ to assisted dying law is contradicted by the data.
The rate of non-voluntary euthanasia has decreased significantly in both the Netherlands and Belgium since assisted dying was permitted by statute.
Assisted dying rates in Dutch-speaking cultures are significantly higher than in non-Dutch cultures, seemingly unrelated to the permissiveness of the jurisdiction’s legal framework.
Benelux country reported assisted dying rates (as a percentage of all deaths)
as at 2014. The three countries have similar assisted dying laws.
Fact file by Neil FrancisPosted on Thursday 7th July 2016 at 10:19pm
Lead author Professor Ezekiel Emanuel discusses the findings of the JAMA study.
Several of the world's foremost researchers in medical end-of-life matters have released a detailed and comprehensive review of the practice of assisted dying in lawful jurisdictions around the world. Published in the Journal of the American Medical Association, it does not support slippery slope hypotheses.
Professors from universities in the USA, the Netherlands and Belgium studied data from government and statutory authority reports, primary scientific studies and other sources to examine how assisted dying has been practiced in different jurisdictions around the world where it is lawful in one form or another: self-administered medication (physician-assisted dying) or physician-administered medication (active voluntary euthanasia).1
Their primary conclusion is that:
"Euthanasia and physician-assisted suicide are increasingly being legalized, remain relatively rare, and primarily involve patients with cancer. Existing data do not indicate widespread abuse of these practices."
Key findings
Key findings include:
Public opinion favouring assisted dying in developed countries has been increasing, or remained stable at high levels of approval.
The trends seem to correlate with decreasing religiosity in Western countries.
The only place where assisted dying approval appears to be decreasing is in eastern Europe, where religiosity has been increasing.
Approval amongst physicians seems to be consistently lower than amongst the public.
Assisted dying occurs everywhere, including juridictions where it is unlawful (as I have previously reported).
Most individuals who choose assisted dying have advanced cancer (as I have previously reported).
Supposedly 'vulnerable' groups are not represented in assisted dying figures at rates any higher than their presence in the overall population.
Numbers of assisted deaths in lawful jurisdictions continue to increase, but represent a tiny minority of deaths.
In jurisdictions where only self-administration is permitted, assisted deaths represent around 0.3% of all deaths.
In jurisdictions where physicians may administer, assisted deaths represent around 3–5% of all deaths.
Assisted deaths for minors and those with dementia are a very small minority of cases (as I have previously reported).
The dominant reasons for requesting assisted death include loss of autonomy and dignity and the inability to enjoy life and regular activities; not physical pain.
Doctors still report that honouring a request for assisted death is emotionally burdensome; not a routine or welcomed option.
"In no jurisdiction was there evidence that vulnerable patients have been receiving euthanasia or physician-assisted suicide at rates higher than those in the general population."
Complication rates
One aspect of the study is worthy of special mention: the small rate of assisted dying procedure complications. The available data suggests that complications may occur more often for self-administered medication than for physician administration:
For self-administration—
Difficulty in swallowing in 9.6% of cases
Vomiting or seizures in 8.8% of cases
Awakening from coma in 12.3% of cases
For physician administration—
Technical problems such as difficulty in finding a suitable vein in 4.5% of cases
Vomiting or seizures in 3.7% of cases
Awakening from coma in 0.9% of cases
This data is however of Dutch practice in the 1990s, before assisted dying was codified in statute—at a time when practice was poorly defined and a range of drugs, including opioids, were widely used. Now, practice is well-defined with almost universal use of barbiturates. The researchers expressly note that these complication rates may well have reduced.
Further, the authors refer to more recent data from Oregon and Washington which indicate very much lower complication rates (in those jurisdictions for self-administration only):
In Oregon, the complication rates are around 2.4% for regurgitation and 0.7% for awakening from coma.
In Washington, the complication rates are around 1.4% for regurgitation, plus a single case of seizure.
The importance of context
It is worth comparing the complication rates of assisted dying procedures with rates for other medical interventions to provide an appropriate context so that they may be realistically interpreted.
For example, a study of common over-the-counter analgesics for short-term pain management2 found that significant adverse effects occurred amongst 13.7% of ibuprofen users, 14.5% of paracetamol useres and 18.7% of aspirin users.
In another example, an anlaysis of primary research about surgical outcomes found that 14.4% had adverse events, almost half of which (47.5%) were moderate to fatal in severity.3
Conclusion
The study is a solid synthesis of research data and indicates that assisted dying is accessed sparingly and in accordance with the intentions of each legislature.
The adverse event rate for assisted dying appears to be substantially lower than the rate of adverse events in the use of common over-the-counter analgesics and in surgery.
References
Emanuel, EJ, Onwuteaka-Philipsen, BD, Urwin, JW & Cohen, J 2016, 'Attitudes and practices of euthanasia and physician-assisted suicide in the united states, canada, and europe', JAMA, 316(1), pp. 79-90.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
Anderson, O, Davis, R, Hanna, GB & Vincent, CA 2013, 'Surgical adverse events: a systematic review', Am J Surg, 206(2), pp. 253-62.
Blog by Neil FrancisPosted on Thursday 12th November 2015 at 5:35am
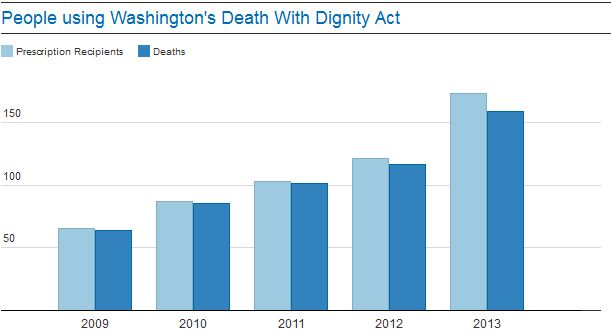
I was browsing the internet the other day checking out commentary on assisted dying in Oregon and Washington state in the USA, and came across an argument in The Guardian—complete with a chart of 'evidence'—that unlike in Oregon, almost all folks who receive a prescription under Washington's Death With Dignity Act (DWDA) die from taking it. 'Eh!?' I thought to myself. I've read all the Washington annual DWDA reports and analysed the data in my own spreadsheets. What The Guardian says is simply not true. How so?
In an editorial on July 18, 2014, The Guardian attempted to estimate the number of people who might use an assisted dying law if it were legalised in the UK. They noted that around a third of Oregonians receiving a prescription under the DWDA died not having taken it. But, they said, "the figures in Washington look quite different. For instance, there isn’t as large a gap in numbers between those who were given prescriptions and those who died." And they offer this chart, which essentially reproduces Figure 2 of Washington's 2013 DWDA annual report, as evidence.
Therein lies a significant problem: the time-poor mistake of grabbing some data out of a report and reproducing it without reading the whole report to understand what the data represents or what it means, and, more particularly, what it doesn't mean.
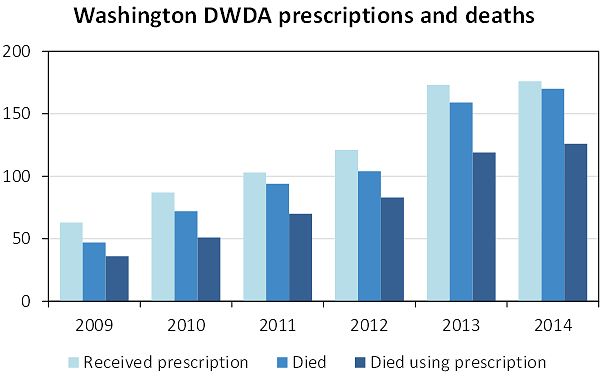
The thing about the Washington DWDA annual reports, when you read them properly, is that they generally report statistics for all people who have qualified under the Act, i.e. have passed all the critieria and had a prescription written. This is different from the Oregon reports, where most of the statistics relate to people who died by ingenstion of their prescription. This can account for some discrepancies between the two states, and caution in comparing certain statistics.
But the bigger issue, and the cause of the misunderstanding of The Guardian, was twofold. Firstly, as explained, the Washington data quoted was for total deaths of DWDA qualifiers, not of deaths by ingestion of the prescription. Secondly, it is longitudinal data for the deaths of DWDA qualifiers who died in any year, allocated to the year of their first qualification under the DWDA: i.e. backdated.
Oregon doesn't report its data in this way, so comparisons cannot be made on that basis. Both states do report the net number of deaths within a calendar year, so that provides a basis for useful comparison. Using this basis, the Washington data looks like this (updated with avialable 2014 data):
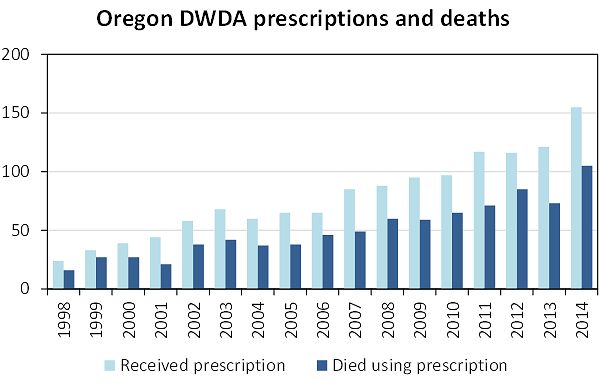
The comparable data from Oregon (without 'Died' because that statistic is not reported in a way that can be compared), looks like this:
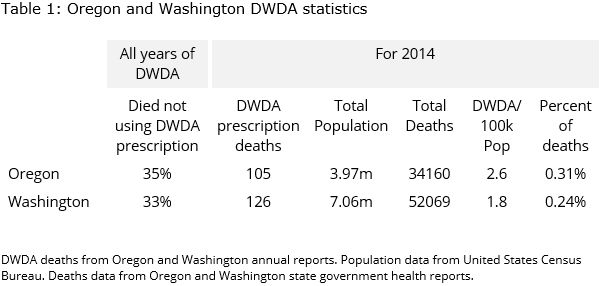
So, Oregon and Washington are indeed quite similar. Overall statistics are:
Nearly the same proportion of those who die in relation to Washington's DWDA but don't use their medication, as do in Oregon. That's quite a different picture from the one created in understandable haste by The Guardian.



 Figure 1: ICU was used in the last 30 days of life
Figure 1: ICU was used in the last 30 days of life Figure 2: Patient was discharged from hospital in the last 30 days of life
Figure 2: Patient was discharged from hospital in the last 30 days of life Figure 3: Dying patient received hospice care at home
Figure 3: Dying patient received hospice care at home Figure 4: The individual died at home
Figure 4: The individual died at home