Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
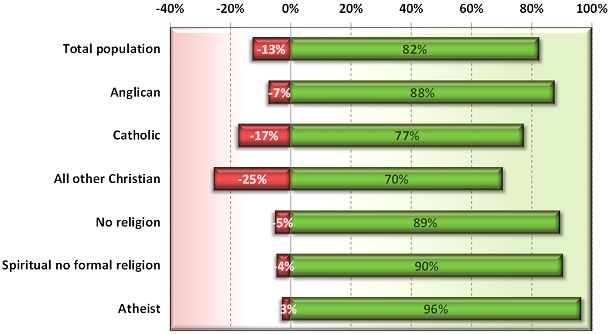
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
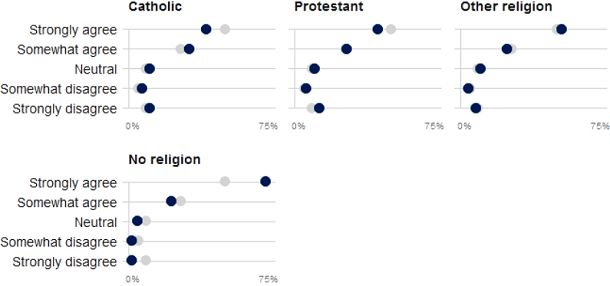
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
Blog by Neil FrancisPosted on Sunday 23rd August 2015 at 10:00pm
ABC journalists Jesse Dorsett and Eleni Roussos recently reported remarks made by the Northern Territory (Australia) Health Minister John Elferink, about the cost of supporting dying patients in the last year of life. Elferink said that dying patients could be personally persuaded to forgo medical treatment specifically in order to have more money available for their grandkids' 'opportunities'. Why is he wrong and what should he do about it?
Stating that "we've pretty much reached the limit of how old we can grow as a species", Minister Elferink estimated that elderly people with terminal illness cost the Northern Territory $1 million in health care costs in the last year of life. Even more astonishingly, he opined that the dying might be persuaded to obligingly shuffle off this mortal coil with the argument that "we can continue treatment but by discontinuing treatment your grandchildren would have a better opportunity" and "think of the work that could be achieved ... in the first year of life with $1 million".
He acknowledged that his remarks would be controversial.
No kidding.
Here are some reader comments from NT News:
"The Elf should be sacked. To say the seniors are a waste of money is abhorrent." — T. Miller
"Watch out Elf, you'll be old one day too." — Elli
"I worked all my life until 69 and paid taxes but judging from your comments us oldies are not worth saving." — Maree
"Hopefully he will lose his seat at the next election having shown us what an uncaring person he is. His statement is an insult to seniors and their loving families too." — Sue
What's wrong with his argument that ill seniors ought to nobly sacrifice themselves at the altar of general public 'good'? Plenty: but let's stick with just three, beyond the obvious fact that Northern Territory seniors are seriously offended by his comments and they vote.
Firstly, this is cheap dog-whistle politics that once again stupidly pitches one Australian against another (remember the infamous 'Leaners versus Lifters' campaign last year?) at the expense of insights and innovative solutions that satisfy everyone's needs.
Secondly, his estimate of the average cost of last-year-of-life medical costs beggars belief.
In a careful analysis of the cost of the last year of hospital care for New South Wales patients, Kardamanidis and colleagues1 found they varied from around $7,000 to $18,000. For the sake of argument, let's use a round figure of $15,000. And, given these are 'hospital' costs (where most dying people end up) but don't cover everything like pharmaceuticals, home care and the like, let's double it to $30,000. That's fairly consistent with figures from the USA, and is likely to be replicated across Australia.
But, heck, the Northern Territory is a vast place with many remote communities, so let's toss in an extra average $20,000 for the Royal Flying Doctor Service on top. That's a total average of $50,000.
Yet John Elferink's 'estimate' is a jaw-dropping twenty times even that generous figure. Is he off with the fairies?
Kardamanidis' study adds another dimension to our insights, too. They found that the average cost of hospital care decreased with old age: $17,927 for 65–74yo; $14,498 for 75–84yo; $10,403 for 85–94yo; and $7,028 for 95+yo. The very elderly dying use hospital services far less than those less old.
The Minister's perceptions and ageist 'formula' for self-sacrifice is seriously at odds with actual evidence.
And thirdly, his superficial, combative assessment quite overlooks excellent and readily-available solutions. It's well-established that higher differential end-of-life healthcare costs are significantly associated with attemps at life-sustaining ICU interventions (e.g. a UK study by Hanchate and colleagues2).
But there's more. An extensive multi-centre USA study by Zhang and colleagues3 reveals that simply by having better conversations with their doctors, advanced cancer patients not only reduced the amount of medical interventions, but achieved better quality of death.
By improving real conversations about the the likelihood of futility versus effectiveness of medical interventions at the end of life, balanced with information about the invasiveness or burden of enduring them, patients themselves can avoid interventions they judge to be of no net value, or even counterproductive.
So, Minister, quit the ill-informed and cheap political shots. Seek informed and practial advice and get on with the job of governing for all Territorians. Implement policies that encourage and facilitate real and meaningful conversations between patients and their doctors at end of life. The health bill will naturally go down for ethically sound—rather than ethical stink-bomb—reasons.
-----
Kardamanidis, K, Lim, K, Da Cunha, C, Taylor, LK & Jorm, LR 2007, 'Hospital costs of older people in New South Wales in the last year of life', Medical Journal of Australia, vol. 187, no. 7, pp. 383-386.
Hanchate, A, Kronman, AC, Young-Xu, Y, Ash, AS & Emanuel, E 2009, 'Racial and ethnic differences in end-of-life costs: why do minorities cost more than whites?', Archives of Internal Medicine, vol. 169, no. 5, Mar 9, pp. 493-501.
Zhang, B, Wright, AA, Huskamp, HA, Nilsson, ME, Maciejewski, ML, Earle, CC, Block, SD, Maciejewski, PK & Prigerson, HG 2009, 'Health care costs in the last week of life associations with End-of-life conversations', Archives of Internal Medicine, vol. 169, no. 5, pp. 480-488.
Update 25th August
Minister Elferink phoned me directly to put his case. We had a respectful if brief conversation (he was in a Parliamentary session). He said that the journalist's report had misrepresented his statements. We agreed that at the very least, the remarks he made were injudicious in the context of end-of-life, and I reiterated that I thought suggesting in any manner that people should give up part of their lives for the economic benefit of others was repugnant. I also reiterated that should the NT Government choose to invest a modest sum in the education of doctors in how to hold respectful, open conversations with patients and in a way that the truly listened to both what was being said as well as left unsaid, that patients would far less often choose futile and burdensome treatments they really didn't want. This would lead to less stress on the patient, their families and healthcare workers, and have the added benefit not only of a better quality of death, but a significantly reduced state healthcare budget.
I hope the Minister takes good evidence and advice on board, and adjusts his stance and the NT Government's approach to medical end-of-life decisions.