Fact file by Neil FrancisPosted on Sunday 13th November 2016 at 1:47am
Assisted dying rates in Dutch-speaking cultures (orange bars) are much higher than elsewhere.
In this whitepaper, Benelux (Belgium, Netherlands and Luxembourg) primary empirical data on assisted dying is analysed — including with new and advanced approaches — to provide fresh insights into contemporary practices. Investigation reveals that the assisted dying rate in Dutch-speaking cultures appears to be uniquely higher than in other cultures irrespective of the permissiveness of the legislative framework, yet is still practiced conservatively.
Download a full copy of the Whitepaper here: PDF (648Kb).
Summary
This new compilation and unique analysis of primary research data from statutory authorities and the peer-reviewed literature provides fresh insights into assisted dying practice in Benelux, including:
Rates of assisted dying in the Netherlands and Belgium have followed an expected sigmoid curve, now beginning to level out.
Several factors have contributed to the higher increase in the Netherlands rate, including recovery from a suppression of cases immediately following statutory reform, a rise in cancer diagnoses, and an increase in granting of assisted dying through new visiting teams launched in 2012.
Both Netherlands and Belgium doctors demonstrate caution if not conservatism when assessing assisted dying requests.
Despite most assisted dying occurring in cases of cancer, fewer than one in ten cancer deaths in the Netherlands and one in twenty in Belgium is an assisted death.
Other conditions such as degenerative neurological, pulmonary and circulatory illnesses each account for a very small proportion of the increase in cases since legalisation in Benelux.
The assisted dying rate in dementia and other mental illness is very low despite controversy around—and a tiny rise in granting of—such cases.
The hypothesis that females or the elderly would be ‘vulnerable’ to assisted dying law is contradicted by the data.
The rate of non-voluntary euthanasia has decreased significantly in both the Netherlands and Belgium since assisted dying was permitted by statute.
Assisted dying rates in Dutch-speaking cultures are significantly higher than in non-Dutch cultures, seemingly unrelated to the permissiveness of the jurisdiction’s legal framework.
Benelux country reported assisted dying rates (as a percentage of all deaths)
as at 2014. The three countries have similar assisted dying laws.
The AMA fails to represent the breadth of physicians perspectives around assisted dying.
This informative Go Gentle Australia video explains why the Australian Medical Association is out of touch with the wider Australian doctor community. Around a third of Australian doctors are members of the AMA.
The AMA currently holds a position of hostility towards assisted dying law reform, as it did against abortion before that was formally legalised. The doctors in this video explain how the AMA does not represent their views on assisted dying in restricted circumstances.
The F filesPosted on Friday 14th October 2016 at 1:21am
BMA House in Tavistock Square, London, home to the British Medical Association since 1925.
The British Medical Association (BMA), in the latest incarnation of its policy on assisted dying (AD), insists that AD must not be legalised in the UK. I argue that its indefensible stance reveals ignorance, incoherence and hubris. It fails to respect the true range of views amongst UK doctors. I expose the comprehensive rot.
The BMA categorically states in its July 2016 policy update on assisted dying:
“The BMA policy … insists that voluntary euthanasia [and] physician-assisted suicide should not be made legal in the UK.” — British Medical Association1
BMA comprehensively out of touch
The BMA claims to represent UK doctors—though fewer than half are members. What is the empirical evidence for UK doctor attitudes toward assisted dying?
In a 2009 survey,2 35% said that AD should definitely or probably be legalised. The same study also found that 35% of UK doctors said AD should definitely not be lawful even in cases of terminal illness. That is, the stance of just 35% of UK doctors was identical to the BMA’s—insisting that it not be lawful, while an equal proportion thought AD could be legalised. “Greater religiosity” was the strongest correlative factor with opposition to lawful AD.
Indeed, numerous studies have found a substantial minority of UK doctors in favour of lawful AD, including results approaching equality with opponents.3 Even a survey commissioned by the UK Catholic Medical Association in 2003 found around 25% of UK doctors in favour of AD and who would practice it if legalised.4
UK doctor support for AD, then, is substantial and hardly restricted to a mere handful of fringe-dwelling medical crackpots.
Ignorant and disrespectful BMA stance
It is untenable that the BMA unilaterally ‘respects’ the views of 35% of UK doctors at the same time as expressly disrespecting the views of another significant cohort. Perhaps as in general politics, its power base is more heavily populated with religious souls: those who have a deeper interest in shaping what options others do and don’t have?
Appalling and trivialised ‘rationale’
Let’s take a look at the five moribund reasons the BMA offers in defense of its institutional opposition to AD and see how they use flapdoodle, fudge, fiction, fear-mongering, flip-flop and hubris to ‘advance’ their position.
“Current BMA policy firmly opposes assisted dying for the following [five] key reasons:”
1. Permitting assisted dying for some could put vulnerable people at risk of harm.
Flapdoodle. Firstly, as I have explained before, the “vulnerable at risk” argument is a rhetorical sham. People ‘at risk’ are by definition ‘vulnerable,’ and would still be so if we wore yellow socks on Wednesdays or outlawed pizza. It has nothing to do with AD being legalised or not.
Fudge. Secondly, the BMA ignores repeated reviews published in the professional literature indicating that supposed harms have not eventuated in jurisdictions with lawful assisted dying. Indeed, the quality of medical practice has improved.
Flip-flop. And thirdly, if ‘risk of harm’ was a sufficient condition to deny patients a particular option, we must equally ban the right to refuse life-saving medical treatment (no matter how unwanted or burdensome) because greedy relatives eyeing off the estate might convince the dying patient to refuse. It’s incoherent to oppose assisted dying, but to support refusal of treatment (as the BMA does), in the face of this identical possibility.
2. Such a change would be contrary to the ethics of clinical practice, as the principal purpose of medicine is to improve patients’ quality of life, not to foreshorten it.
Fudge. Medicine has a number of primary purposes. Relief of suffering is one.5 That may come into conflict with another purpose, “the avoidance of premature death and the pursuit of a peaceful death” (which itself has internal conflicts). A dying individual may herself believe that an AD would not be premature, and whose peaceful nature is vastly preferable to continued intolerable and unrelievable suffering.
3. Legalising assisted dying could weaken society's prohibition on killing and undermine the safeguards against non-voluntary euthanasia. Society could embark on a 'slippery slope' with undesirable consequences.
Fear-mongering. Non-voluntary euthanasia (NVE) is currently illegal. It remains illegal even when AD is legalised. The BMA therefore incoherently conjectures that NVE doesn’t occur while it’s illegal (before AD legalisation), but might occur while it is still illegal (after AD legalisation).
Fiction. There are no current ‘safeguards’ against NVE as the BMA statement implies. It is practiced in secret. There are no statutory requirements or reporting standards as there are for AD (where legal). Research clearly demonstrates that NVE occurs everywhere, including the UK. Further, the rate of NVE has significantly decreased in the Netherlands and Belgium since their AD statutes came into effect.
4. For most patients, effective and high quality palliative care can effectively alleviate distressing symptoms associated with the dying process and allay patients' fears.
Flapdoodle. The BMA says “effective … palliative care can effectively alleviate…”: another circular, self-‘proving’ argument.
Hubris. The BMA acknowledges here—as unarguably established in the professional literature—that palliative care can’t help everyone. And that’s precisely what assisted dying law reform is about: for people that palliative care can’t help. But the BMA brushes them under the carpet.
5. Only a minority of people want to end their lives. The rules for the majority should not be changed to accommodate a small group.
Flip-flop. In ‘reasons’ 1 and 3 above, the BMA speculates that too many people will die if AD is legalised. Here is it arguing that too few will. Which is it? Too many or too few? The argument also ignores the international evidence that dying individuals (and their loved ones) experience profound relief merely from knowing that AD is available, even if they don’t pursue it. That itself is good palliative care.
Hubris. And if “not changing the majority's rules to accommodate a small group” were a gold standard as the BMA argues, then there would be no leglisation to (a) ensure facilities access to people with a disability, (b) outlaw discrimination on the basis of race or religion, or (c) allow same-sex marriage: all enshrined in law in the UK.
Hubris argues for ignoring the BMA itself
If, as the BMA argues, we should override the wishes of a group on the basis of its small size, it’s pertinent to consider the size of the UK doctor population: around 0.4% of the total. By comparison, in jurisdictions where AD is legal, around 0.3% (Oregon) to 3.8% (Netherlands) ultimately choose an assisted death.
If we are to ignore 0.3%–3.8% of the population because it’s ‘too small,’ we must equally ignore 0.4% of it. This, by the BMA’s own argument, would be reason to force it to support AD because that’s what the majority (UK population) favour. After all, “the rules for the majority should not be changed to accommodate a small group [of doctors].”
Of course most of us recognise, unlike the BMA, that this is not a ‘popularity contest.’ A stance of neutrality would demonstrate respect for deeply-held views across the spectrum.
Conclusion
The British Medical Association demonstrates profound ignorance about the available evidence, and about UK doctor attitudes. It resorts to fear-mongering speculation, fudge, fiction, flapdoodle, flip-flop and hubris to maintain its indefensible opposition to assisted dying.
The BMA’s stance does a great disservice to the British people. It’s an embarrassment to professional doctors regardless of their stance on assisted dying. The policy deserves to be entirely scrapped, and one of neutrality adopted in its place.
Seale, C 2009, 'Legalisation of euthanasia or physician-assisted suicide: survey of doctors' attitudes', Palliative Medicine, 23(3), Apr, pp. 205-212.
McCormack, R, Clifford, M & Conroy, M 2011, 'Attitudes of UK doctors towards euthanasia and physician-assisted suicide: a systematic literature review', Palliative Medicine, 26(1), pp. 23-33.
Catholic Medical Quarterly 2003, 'Euthanasia and assisted suicide: Results of survey of doctors attitudes', Catholic Medical Quarterly, May, pp. 1-3.
Hastings Center Report 1996, 'The goals of medicine. Setting new priorities', The Hastings Center Report, 26(6), pp. S1-27.
The F filesPosted on Wednesday 5th October 2016 at 10:21pm
Palliative Care Australia's position statement on assisted dying.
I’ve written previously about palliative care specialists trying to filibuster assisted dying law reform. In this F file, I reveal how Australia’s peak body for palliative care (PC), Palliative Care Australia (PCA), segues from a state of ignorance to its own filibuster that would stall assisted dying choice.
First up, let me say that I hold deep admiration for the generally excellent services PC specialists provide at the bedside. I believe that PC deserves strong support and good funding. The peak body’s leadership in regard to its stance on assisted dying, however, is of a dramatically lower calibre.
Revised policy statement
In PCA’s latest incarnation of its Position Statement on ‘Euthanasia and physician assisted suicide’,1 the organisation says that:
“Public discussion and policy development on issues related to euthanasia and physician assisted suicide should be informed by research. There is insufficient research into euthanasia and physician assisted suicide.” — Palliative Care Australia, Position Statement
One can only agree wholeheartedly with the first sentence. Of course public discussion and policy development should be informed by research wherever possible.
The filibuster
And there follows the filibuster rub — PCA unequivocally claims that there is insufficient research. The logical consequence of PCA's juxtaposition is that we ought to muzzle public discussion and policy development because, PCA alleges, there is insufficient research to inform it.
Certainly in terms of Australia there are only a handful of published studies into attitudes and practices. But assisted dying is illegal in Australia. There are very substantial ethical and legal issues when it comes to conducting research.
Who is PCA to claim "insufficient research"?
PCA is the peak body for PC, a specific discipline within medicine that represents (well-paid) doctors. It runs a staffed office in Fyshwick ACT, and is overseen by a Board and Executive. It has a key purpose of lobbying in the halls of power in the Federal Parliament, and, presumably on the basis of the statement above, has a goal of ensuring that government PC policy (and funding) is informed by research. You'd think it might have some resources and connections to go looking for some research evidence.
A revealing comparison
In comparison, I conduct my assisted dying law reform work on a completely pro-bono basis, as a single individual, in my spare time. I have a formal literature collection on end-of-life decision making, including assisted dying, of currently over six thousand articles. I’m not talking about mere opinion published in the media: I’m talking about articles published in professional journals and in official government and agency reports.
I just ran a quick check across my database, looking for items specifically in respect of assisted dying (not medical or palliative care in general) in the Netherlands, Belgium and Oregon, where assisted dying has been legal for some time. Here’s what I found.
In respect of assisted dying the Netherlands I hold 366 journal articles and 25 official reports. For Belgium, I hold 152 journal articles and 11 official reports. And for Oregon I hold 144 journal articles and 32 official reports.
That’s a total of 662 journal articles and 68 official reports in respect of three lawful assisted dying jurisdictions. And that doesn’t count any holdings of book chapters, conference papers and the like. The journal article count will be somewhat overstated because a minority of journal papers are about more than one lawful jurisdiction (e.g. the Netherlands and Belgium). So let’s estimate that downwards to, say, a mere 400 journal articles.
That’s an abundance of evidence from and review about jurisdictions where assisted dying is legal. Could we always know more about assisted dying? Sure.
Double standards when it comes to evidence
We could also know a lot more about PC. I recently asked PCA for a simple but critical headline statistic — one you’d think was necessary to inform policy about PC resources and funding: “what proportion of Australians who experience a non-sudden death (i.e. deaths where PC might be relevant) actually receive PC?”
PCA kindly responded, but the answer in a nutshell was “we don’t know.”
But I wouldn't suggest for a moment that we muzzle “public discussion and policy development on issues related to PC” because the peak body hasn't done enough research to calculate (or even estimate) a fundamental policy-informing statistic.
Conclusion
The Australian community would be better served if PCA acquainted itself with the extensive available literature on assisted dying in lawful jurisdictions (as well as headline PC statistics), and dropped its inappropriate filibuster.
References
Palliative Care Australia 2016, Euthanasia and physician assisted suicide: Position statement, viewed 1 Sep 2016, <http://palliativecare.org.au/download/2448/>.
Blog by Neil FrancisPosted on Saturday 3rd September 2016 at 4:44am
Mr Steve Jalsevac of the Catholic LifeSiteNews blog who made a shocking and vile attack.
I recently exposed (another) piece of misinformation published by LifeSiteNews, and wrote courteously to them to request withdrawal of the offending article. While I wasn’t hopeful the request would be accepted, I wasn’t prepared for the shocking and vile response I received.
Exposing bull about assisted dying is a key purpose of DyingForChoice.com and it will continue to do so as long as bull is published or publicly spoken, and especially when it makes claims or generates innuendo that is at odds with the readily-available facts, as a smokescreen for fundamentally religious objections.
The specific request to withdraw
In a recent article I factually rebutted the allegation by Mr Brad Mattes that there is suicide contagion (from assisted dying to general suicide) in Belgium, in addition to other statements that were wrong in fact in his opinion piece published by LifeSiteNews. I wrote a courteous letter to the editor of LifeSiteNews to point out the errors and to seek withdrawal of the article.
My full email to LifeSiteNews
Dear LifeSiteNews,
Clearly we are on different sides of the assisted dying conversation. I’m sure that we can mutually appreciate that different people bring different perspectives and apply some largesse in terms of world views.
However, one must draw the line (as your primary Principle does and upon which I think we agree) at the publication of information, however accidental, on your website that is in places fundamentally misleading and elsewhere quite false.
In this regard may I request that you withdraw the article by Mr Brad Mattes, Assisted suicide no longer just for the terminally ill, that contains multiple errors of evidential fact as well as fundamentally misleading statements, as I point out in this post?
Kind regards
Neil Francis
The shocking response
A firm believer in courteous debate even when one disagrees profoundly on important matters, I thought the most likely outcome would be a polite letter declining my request. But I received instead this response from LifeSiteNews Managing Director, Mr Steve Jalsevac.
Full response by Mr Steve Jalsevac of LifeSiteNews
Dear Neil,
I find it somewhat amusing that an advocate for legislation to allow people to kill themselves is demanding that we withdraw an article for supposedly publishing "misleading" or "false" information.
After many years of covering organizations such as yours which, typically cruelly manipulate vulnerable persons, violate or liberally interpret laws, understate their longer term objectives, have an extremely unhealthy and dangerous satisfaction in personally seeing people die before their eyes before their natural time, devastate family members whose loved ones had, unknown to them, been guided to kill themselves, and who have such perverse and wrong views on Christian beliefs and much more, I find it despicable that you would be so concerned about supposed accuracy. You, sir, are a hypocrite of the very worst kind.
It is our view that you should be behind bars for what you advocate and for your dangerous manipulation of vulnerable persons.
I realize that you will not agree with anything that I write given how blinded your conscience and intellect have become by your death preoccupation. So, I just conclude that your claims, views and interpretations are all rejected because no one should trust anything that you say or do on this subject.
Steve Jalsevac
LifeSite
Who is LifeSiteNews, anyway?
LifeSiteNews is an online blog established by the conservative Christian Campaign for Life Coalition. It promotes that it “emphasizes the social worth of traditional Judeo-Christian principles.” Its principles are all very courteously worded and sound “respectful” (its principles expressly use that word several times) whilst indicating that it is a pro-life blog.
I’ve read its articles on assisted dying for several years and have not found a single one that is at odds with the position of the Vatican. That’s hardly surprising.
LifeSiteNews publishes a significant proportion of articles about the Catholic Church, as is its right. It is also the sole publisher of Faithful Insight, in its own words “hard-hitting,” “100% faithful” and “fearless Catholic news coverage from the Vatican and beyond.” I argue strongly for the right to publish material of faith. That is not a source of complaint. (Fair disclosure—I’m agnostic.)
LifeSiteNews' hard-hitting and 100% Catholic-faithful publication.
And, Mr Jalsevac gives a clear indication that he’s at the 'Old School' end of the Catholic spectrum. He admires in multiple blogs the writings of conservative African Catholic Bishop Robert Sarah, noting John Paul II’s teachings as “definitive” and expressing disappointment in the current Pope. And that's entirely his right I again affirm.
Mr Jalsevac’s editor-in-chief, Mr John-Henry Westen has also published a number of articles critical of Pope Francis, also referring to previous Popes as more authoritative.
What do they claimto stand for?
LifeSiteNews’ first principle, in full, is this:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.”—LifeSiteNews.com
Mr Jalsevac's response highlights these claimed principles in stark relief by comprehensively breaching them.
The statements Mr Jalsevac makes about me are vile. And false. While I’m calling out his blogs’ misinformation for what it is, he’s calling for me personally to be thrown in jail for sins he falsely thinks I’ve committed. That’s squarely known as the ad hominem attack: attacking the person rather than the argument. It conveniently provides him with the excuse to totally ignore solid evidence that contradicts his beliefs.
Interestingly, an article by LifeSiteNews Editor Mr Westen quotes Pope Francis as saying,
“We Catholics have some — and not some, many — who believe in the absolute truth and go ahead dirtying the other with calumny, with disinformation…”—Pope Francis.
Quite.
Conclusion
LifeSiteNews is an 'Old School' Catholic blog, and, I argue, has every right to be.
However, it has demonstrated by publishing multiple articles containing serious errors of fact as well as highly misleading statements, and by a gratuitous ad hominem attack on someone pointing this out, that it is not interested in evidence, reason or even civility as it claims. In my view it has unambiguously demonstrated itself to be a biased and unreliable Catholic source on matters of assisted dying.
I will continue to call out misinformation in LifeSiteNews when I see it.
Blog by Neil FrancisPosted on Sunday 28th August 2016 at 12:58am
Brad Mattes' blog containing misleading and evidentially false statements.
The latest misinformation employed by assisted dying opponents is to imply that Belgium’s general suicide rate is high as a consequence of its assisted dying law: i.e. to argue the discredited 'suicide contagion' line which has in the past been peddled about the USA state of Oregon. I have demonstrated that it was false in Oregon, and I equally demonstrate here that it's false in Belgium.
Mr Brad Mattes recently published emotional anti-assisted-dying nonsense in LifeSiteNews. (LifeSiteNews is a Canadian blog site that was established by the conservative Christian Campaign for Life Coalition and which has a primary principle of promoting “traditional Judeo-Christian principles”. Mr Mattes is radio host for Ohio’s Life Issues Institute, an anti-abortion lobby group established by conservative American John C. Willke who claimed that women’s bodies were resistant to pregnancy as a result of rape.)
Putting on the misinformation running shoes
In his blog Mr Mattes quickly establishes a practice of communicating misinformation by first claiming that assisted dying laws have “devastating effects” around the world including Japan and Albania—which don’t have such laws.
He then sprints onwards to the ‘650 babies euthanized in the Netherlands’ claim—which I have already comprehensively exposed as fake in the Journal of Assisted Dying—and then onto the bogus claim that the Netherlands has descended into a mire of ‘killing’ without the patient’s ‘consent,’ contrary to empirical evidence I've published that such actions occur around the world regardless of assisted dying laws, and which have decreased significantly in the Netherlands and Belgium since their assisted dying statutes came into effect in 2002.
Let’s add fries to that
Having served up a lot of fat and salt that might appeal to those on a fast-food anti-assisted-dying diet, he then offers the unqualified statement:
“By the way, Belgium has the second-highest suicide rate (nonrelated to euthanasia) in Western Europe.” — Brad Mattes
The ‘informational’ consequence is unequivocal: by Mr Mattes failing to contextualise this ‘incidental factoid’ in any way, the reader is destined to deduce that it is Belgium’s euthanasia law that causes Belgium’s suicide rate to be the second-highest in Western Europe. In other words, Mr Mattes is another poorly-informed commentator using the 'suicide contagion' line.
But what are the facts?
Depending on the source and year of data, one can certainly argue that Belgium’s general suicide rate is the second-highest in Western Europe. Setting aside for now the serious question of why it is valid to exclude all of the world’s other countries from the comparison, WorldLifeExpectancy.com reports figures that were published in 2014 (Table 1).
Table 1
Country
Suicides*
Finland
15.11
Belgium
14.64
Iceland
14.06
France
12.84
Austria
11.87
Sweden
11.43
Ireland
11.06
Germany
9.59
Switzerland
9.56
Norway
9.28
Denmark
9.19
Luxembourg
9.14
Netherlands
8.54
Portugal
8.49
Turkey
7.92
UK
6.28
Malta
5.75
Spain
5.23
Italy
4.76
Greece
3.86
* Suicides per 100k population, age-adjusted
The table includes all the countries in the wider definition of “Western Europe”, bar four: no suicide statistics are published for Liechtenstein, Monaco, Andorra or San Marino.
As you can see, Belgium is indeed the second-highest. But this begs the question:
If the reason Belgium is the second-highest is due to its assisted dying law, how come Finland, which Mr Mattes doesn't mention by name and which has no such law, is higher?
It also begs the question:
If assisted dying law were the fundamental cause of a high general suicide rate, how come Switzerland (statute since 1942), Luxembourg (statute since 2009) and the Netherlands (practice since the early 1980s and statute since 2002) have rates that are muchlower, all key facts that Mr Mattes also fails to mention?
These are of course indications that the factoid has been included as a cherry-picked morsel of 'proof' because it sounds so compelling as a throw-away sentence amongst the other (false) statements.
But wait, there’s more
We can go further than merely wondering about the country comparisons, by comparing Belgium’s general suicide rate before and after assisted dying law reform. A critical step in establishing causation is to first establish correlation. If there is no correlation, there can be no causation.
Published OECD data shows that in 2013 (the most recent available data), Belgium’s general suicide rate was 16.7 per 100,000 population. What was it before their 2002 law reform? Well in 2000 it was 20.5, in 1990 it was 19.2, … you get the idea.
Has Belgium’s general suicide rate soared (or even increased modestly) since their 2002 assisted dying law came into effect? No. It’s dropped. Indeed, the slight downward trend apparent before the statute came into effect in 2002 has accelerated downward since (Figure 1).
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Even the headline is misleading
Mr Mattes fails to point out in his blog that assisted dying statutes in Benelux countries (Belgium, the Netherlands and Luxembourg) never restricted access to only the 'terminally ill,' that is, those imminently dying. He also fails to point out that USA states whose laws do restrict assisted dying to the terminally ill—most notably Oregon and Washington—have not changed their statutes in this regard since they came into effect.
Therefore, his headling implying that lawful jurisdictions have broadened their laws from 'only the terminally ill' is also wrong.
Conclusion
Mr Mattes makes multiple false and misleading claims and it’s easy to see his opinion for what it is: an emotional dump that fails to engage with and indeed flies in the face of actual evidence. The latest 'suicide contagion' implication, that assisted dying law causes Belgium’s general suicide rate to be the “second-highest in Western Europe” is evidentially false.
I call on LifeSiteNews to withdraw Mr Mattes' article because it breaches their primary principle:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.” — LifeSiteNews
Summary of facts
Belgium's general suicide rate is one of the higher ones in Western Europe. However:
At least one country without an assisted dying law has a higher suicide rate, inconsistent with 'suicide contagion' theory.
Other Western Europe countries with assisted dying laws have suicide rates much lower than Belgium's, also at odds with 'suicide contagion' theory.
But the clincher is that the suicide rate in Belgium has dropped, not risen, since their 2002 assisted dying law came into effect.
In this interview segment, Dutch Professor Theo Boer self-identifies as a voluntary euthanasia sceptic.
I interviewed Dutch Professor Theo Boer—Social Professor of Ethics at Theological University, Kampen, the Netherlands, and a Dutch Euthanasia Committee ethicist—about the Netherlands' assisted dying law.
He volunteers that prior to joining a Euthanasia Committee he was an assisted dying sceptic, and remains so.
And yet he warmly endorses the Dutch leglislative model as a good one for other jurisdictions to emulate, a position that he says has become more clear with experience.
Blog by Neil FrancisPosted on Wednesday 3rd August 2016 at 4:15am
Mr Max Bromson (seated) at Parliament House Canberra in June 2014. He died not long afterwards.
Assisted dying critic Mr Paul Russell has done it again. I’m beginning to think that he’s a tremendous asset to the pro-assisted-dying movement. Why would I say that?
Well, this time his pronouncements appear in National Right To Life News, the online newspaper of the USA Catholic-founded National Right To Life Committee, and in which Mr Russell represents ‘HOPE,’ his anti-euthanasia lobby platform founded by the Australian Family Association—itself Catholic-founded and backed.
The complaint
In his opinion piece, Mr Russell complained that Mr Max Bromson of Adelaide, Australia, who ended his own life after a long period of serious suffering from advanced cancer, lived far longer than his doctors had estimated.1
“That he outlived his diagnosis by more than four years confirms the observation that qualifying periods in euthanasia and assisted suicide about ‘six months to live’ or similar, are really meaningless.” — Paul Russell
The pro-assisted-dying message
Mr Russell, in a single sentence, unequivocally demolishes the foundation of his own arguments in opposition to legalising assisted dying. He is a huge fan of the ‘vulnerable’ argument: that once legalised, people will quickly be pressured into assisted dying.
If his ‘vulnerable’ argument held true (a hypothesis that peer-reviewed scientific research contradicts), those with the means to peacefully end their lives would do so. And they wouldn’t take four years to think about it.
By explicitly pointing out that Mr Bromson had survived for much longer than expected (as fellow assisted-dying critic Mr Wesley Smith pointed out in another case), Mr Russell directly disproves the rhetoric of his ‘vulnerable’ argument.
People will quickly end their own lives... but survive far longer than expected: It's a spectacular flip-flop.
Conclusion
Thanks, Mr Russell, for pointing out that people don’t want to die—that they live as long as they can possibly bear it—and disproving your own nonsense. Keep up the good work!
-----
Footnote: Blind ignorance?
I’m also curious as to whether Mr Russell advances misinformation in blind ignorance, or whether the situation is worse. Who can say?
I have on a number of occasions explained simply and clearly why the west-coast-USA state assisted dying laws require that for the patient to qualify for assisted dying, one of the conditions is that the patient’s doctor must assess that the patient is likely to die within six months.
The reason is not that those with five months to live are deserving of the choice, but those with ten months to live are not, as Mr Russell bizarrely assumes.
The very important outcome is that when the doctor makes that assessment, the patient then automatically qualifies for free hospice care. It takes monetary considerations out of the equation, which is important in the context of the expensive USA healthcare system.
So, Mr Russell demonstrates profound ignorance at best by opining that the prognosis of time remaining must be superbly accurate, when it can’t be except possibly in the last days.
It’s about quality of life, not quantity; framed by hospice care being readily and freely available.
Fact file by Neil FrancisPosted on Thursday 7th July 2016 at 10:19pm
Lead author Professor Ezekiel Emanuel discusses the findings of the JAMA study.
Several of the world's foremost researchers in medical end-of-life matters have released a detailed and comprehensive review of the practice of assisted dying in lawful jurisdictions around the world. Published in the Journal of the American Medical Association, it does not support slippery slope hypotheses.
Professors from universities in the USA, the Netherlands and Belgium studied data from government and statutory authority reports, primary scientific studies and other sources to examine how assisted dying has been practiced in different jurisdictions around the world where it is lawful in one form or another: self-administered medication (physician-assisted dying) or physician-administered medication (active voluntary euthanasia).1
Their primary conclusion is that:
"Euthanasia and physician-assisted suicide are increasingly being legalized, remain relatively rare, and primarily involve patients with cancer. Existing data do not indicate widespread abuse of these practices."
Key findings
Key findings include:
Public opinion favouring assisted dying in developed countries has been increasing, or remained stable at high levels of approval.
The trends seem to correlate with decreasing religiosity in Western countries.
The only place where assisted dying approval appears to be decreasing is in eastern Europe, where religiosity has been increasing.
Approval amongst physicians seems to be consistently lower than amongst the public.
Assisted dying occurs everywhere, including juridictions where it is unlawful (as I have previously reported).
Most individuals who choose assisted dying have advanced cancer (as I have previously reported).
Supposedly 'vulnerable' groups are not represented in assisted dying figures at rates any higher than their presence in the overall population.
Numbers of assisted deaths in lawful jurisdictions continue to increase, but represent a tiny minority of deaths.
In jurisdictions where only self-administration is permitted, assisted deaths represent around 0.3% of all deaths.
In jurisdictions where physicians may administer, assisted deaths represent around 3–5% of all deaths.
Assisted deaths for minors and those with dementia are a very small minority of cases (as I have previously reported).
The dominant reasons for requesting assisted death include loss of autonomy and dignity and the inability to enjoy life and regular activities; not physical pain.
Doctors still report that honouring a request for assisted death is emotionally burdensome; not a routine or welcomed option.
"In no jurisdiction was there evidence that vulnerable patients have been receiving euthanasia or physician-assisted suicide at rates higher than those in the general population."
Complication rates
One aspect of the study is worthy of special mention: the small rate of assisted dying procedure complications. The available data suggests that complications may occur more often for self-administered medication than for physician administration:
For self-administration—
Difficulty in swallowing in 9.6% of cases
Vomiting or seizures in 8.8% of cases
Awakening from coma in 12.3% of cases
For physician administration—
Technical problems such as difficulty in finding a suitable vein in 4.5% of cases
Vomiting or seizures in 3.7% of cases
Awakening from coma in 0.9% of cases
This data is however of Dutch practice in the 1990s, before assisted dying was codified in statute—at a time when practice was poorly defined and a range of drugs, including opioids, were widely used. Now, practice is well-defined with almost universal use of barbiturates. The researchers expressly note that these complication rates may well have reduced.
Further, the authors refer to more recent data from Oregon and Washington which indicate very much lower complication rates (in those jurisdictions for self-administration only):
In Oregon, the complication rates are around 2.4% for regurgitation and 0.7% for awakening from coma.
In Washington, the complication rates are around 1.4% for regurgitation, plus a single case of seizure.
The importance of context
It is worth comparing the complication rates of assisted dying procedures with rates for other medical interventions to provide an appropriate context so that they may be realistically interpreted.
For example, a study of common over-the-counter analgesics for short-term pain management2 found that significant adverse effects occurred amongst 13.7% of ibuprofen users, 14.5% of paracetamol useres and 18.7% of aspirin users.
In another example, an anlaysis of primary research about surgical outcomes found that 14.4% had adverse events, almost half of which (47.5%) were moderate to fatal in severity.3
Conclusion
The study is a solid synthesis of research data and indicates that assisted dying is accessed sparingly and in accordance with the intentions of each legislature.
The adverse event rate for assisted dying appears to be substantially lower than the rate of adverse events in the use of common over-the-counter analgesics and in surgery.
References
Emanuel, EJ, Onwuteaka-Philipsen, BD, Urwin, JW & Cohen, J 2016, 'Attitudes and practices of euthanasia and physician-assisted suicide in the united states, canada, and europe', JAMA, 316(1), pp. 79-90.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
Anderson, O, Davis, R, Hanna, GB & Vincent, CA 2013, 'Surgical adverse events: a systematic review', Am J Surg, 206(2), pp. 253-62.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
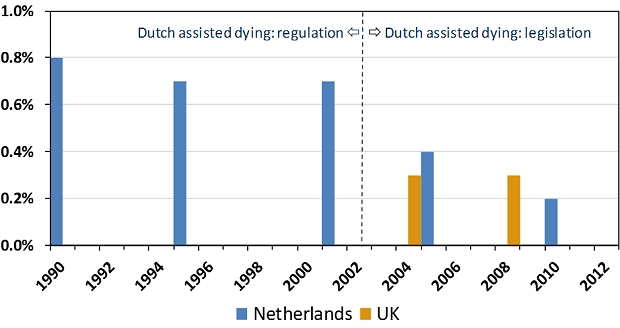
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.


 Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Figure 1: The Belgium general suicide rate before and after assisted dying law reform