Blog by Neil FrancisPosted on Tuesday 8th March 2016 at 7:53pm
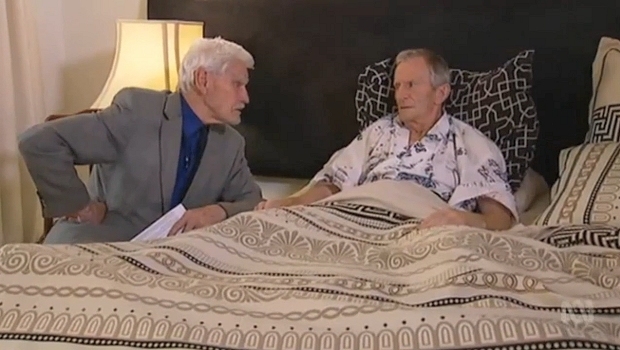
Dr Syme consults with Mr Bernard Erica (ABC Australian Story)
Australia's Medical Registration Board (AHPRA) has told Dr Rodney Syme that he is a serious danger to patients.
Dr Rodney Syme, who occasionally provides advice and medication for dying patients to give them control over their dying process, has been reprimanded by Australia's Medical Registration Board (AHPRA) for posing a 'serious danger' to such patients. The story has been reported widely in the media.
On ABC's Australian Story on Monday night, "My conscience tells me", patient Mr Bernard Erica clearly volunteers that this is utter nonsense, and that like former journalist Mr Steve Guest, who Dr Syme also provided advice and medication to control the end of his life, Mr Erica in no way felt Dr Syme was a threat of any kind. Indeed, like Mr Guest, he has experienced profound and lasting relief from the very knowledge he would have control if and when the time for him came.
Mr Erica's GP, who was aware of and seemed initially supportive of Mr Erica's stance and Dr Syme's advice and medication, lodged a complaint with AHPRA when the ABC's Australian Story contacted him (the GP) for an interview in relation to the case, it was explained on Australian Story. Did this doctor suddenly feel frightened into 'protecting his own arse'?
Coroner's Court data shows that 8.5% of suicides in Victoria are the result of dying patients in extremis being denied the right to a peaceful, doctor-assisted death.
AHPRA need to hear from ordinary Australians, and doctors, that they disagree with the stance it has taken in relation to Dr Syme's careful and compassionate consultations with dying patients. Indeed, to oppose careful and considered medical assessment that providing control is the only way for this particular patient to obtain relief from intolerable psychological suffering—of the State's refusal to allow rational and deeply valued paths to death—is to condemn such patients to a high chance of violent and undignified suicide.
In a key submission to the Victorian Parliament's current inquiry into end-of-life choices, the Coroner's Court of Victoria reported that, after intensive and exquisitely careful analysis, rejecting any equivocal cases, 8.5% of suicides in Victoria are of dying persons experiencing unrelievable and intolerable suffering, and for whom current law does not provide a compassionate and peaceful doctor-assisted death.
By censuring doctors who provide patient choice, it is my view that AHPRA becomes complicit in violent suicides amongst the terminally ill. Thus it is AHPRA and not Dr Syme who represents a 'serious danger' to terminally ill patients.
By reprimanding Dr Syme for his careful and considered private medical practice and for placing additional conditions on his medical license, it is my view that AHPRA becomes complicit in violent suicides amongst the terminally ill. Thus it is AHPRA and not Dr Syme who represents a 'serious danger' to terminally ill patients.
I wrote to AHPRA to express my displeasure at their failure to recognise contemporary community standards, which are enormously in favour of providing terminally ill people the right to a peaceful, doctor-assisted death. Here is what I said.
Dear AHPRA,
I write to express my dismay, along with millions of Australians, at your hostile attitude towards Dr Rodney Syme and your farcical claim that he is a danger to patients. Clearly, you are mired in nineteenth century medical paternalism and are out of touch with contemporary Australian attitudes about having control over one's death in the face of intolerable and unrelievable end-of-life suffering.
Dr Syme will speak for himself of course. But I will also say that having worked with Dr Syme for years, NEVER ONCE in my experience has his "primary intention " (as you put it) been for his patient to end their life when he provides advice and medication. He provides GOOD PALLIATIVE CARE: relieving intolerable psychological suffering. Many of his patients never take the medication.
Please lift your game and modernise. Dr Syme is giving patients control to live better, not inciting them to die: a choice between ways of dying, not between living and dying.
Neil Francis
I urge you to write to AHPRA as well, which you can do here. Scroll down the page to use the web form.
Fact file by Neil FrancisPosted on Thursday 28th January 2016 at 1:30am
Around the world, doctors help patients with assisted dying, regardless of whether it is legal in their jurisdiction or not.
For example, in Australia, where assisted dying is illegal, research reveals that assisted dying is widely practiced. Many Australian nurses have collaborated with doctors to provide assisted dying, and have occasionally even done so without consulting a doctor (Kuhse & Singer 1993). Nurses in New Zealand also provide assisted dying, sometimes without consulting a doctor (Malpas, Mitchell & Koschwanez 2015; Mitchell & Owens 2004).
"Euthanasia is common. It's practiced out of sight, under wraps, no regulation, no rules, no supervision." Prof. Peter Baum (Baum 2001)
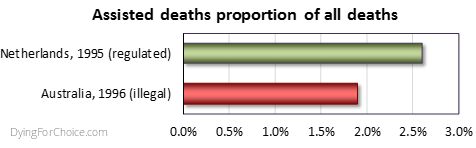
Professor Baum's statement is borne out by scientific research. A national survey of Australian doctors in 1996 found that 1.9% of deaths were the result of voluntary euthanasia (VE) or physician-assisted dying (PAD) (Kuhse et al. 1997). By comparison, the rate in the Netherlands in 1995 (the closest year of empirical research data) was 2.6% (Onwuteaka-Philipsen et al 2012). The rate of medically assisted deaths in Australia, where the practice is illegal, was three quarters the rate of the Netherlands, where the practice is legal.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Forms of medically assisted dying have been found to occur not only in Australia (and in the Netherlands where it has been lawful for decades), but in Belgium prior to its law reform (Chambaere et al. 2015); Switzerland, Denmark, Sweden and Italy (van der Heide et al. 2003); the UK (Seale 2009a; Seale 2009b); the USA (Back et al. 1996; Bonn 2000; Emanuel, Fairclough & Clarridge 1996; Lachman 2010; Schwarz 2003; Schwarz 2004); France (Riou et al. 2015); Norway (Forde & Aasland 2014; Forde, Aasland & Falkum 1997); and even in conservative Greece (Voultsos, Njau & Vlachou 2010); Northern Ireland (McGlade 2000) and Pakistan (Imran et al. 2014).
Indeed, "euthanasia is performed worldwide, regardless of the existence of laws governing it" (Gastmans et al. 2006), "in all countries studied" (Muller, Kimsma & Van Der Wal 1998), "albeit in a secretive manner" (Rosenfeld 2000), "in the privacy of their [doctor-patient] relationship" (Cassell 1995), with repeated involvement of some physicians (Smith 2007), and frequent failure to adhere to high standards when illegal (Emanuel et al 1998).
Even Dr Brendan Nelson, while President of the Australian Medical Association, acknowledged that he had helped hasten the death of a patient. He stated that in the "2 percent of cases" where there was no hope of recovery, that "patients, their families and their doctors make those decisions [for euthanasia]" though clandestinely, because "technically it would be illegal" (Nelson 1995).
AMA's President, Brendan Nelson, in 1995.
The evidence is irrefutable: there is underground assisted dying worldwide and it demonstrates that there is a profound need for assisted dying law reform to allow dying patients the right to seek a peaceful hastened death, and to protect doctors and nurses who provide that assistance. Law reform would also force assisted dying from the dark shadows, creating transparency and accountability around the process, which would then be open to discussion and improvement if required.
Intolerable and unrelievable patient suffering drives underground assisted dying across the world in jurisdictions where it is illegal, with no standards of practice or transparent oversight.
References
Back, AL, Wallace, JI, Starks, HE & Pearlman, RA 1996, 'Physician-assisted suicide and euthanasia in Washington State: Patient requests and physician responses', JAMA, vol. 275, no. 12, pp. 919-925.
Baum, P 2001, ABC News, TV broadcast 23 Jan, ABC, Sydney.
Bonn, D 2000, 'Support for euthanasia falls as care of dying patients improves', The Lancet Oncology, vol. 1, no. 3, p. 133.
Cassell, EJ 1995, 'Treating the patient's subjective state', Pain Forum, vol. 4, no. 3, pp. 186-188.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, vol. 372, no. 12, pp. 1179-1181.
Douglas, C, Kerridge, IH, Rainbird, KJ, McPhee, JR, Hancock, L & Spigelman, AD 2001, 'The intention to hasten death: a survey of attitudes and practices of surgeons in Australia', Medical Journal of Australia, vol. 175, no. 10, pp. 511-515.
Emanuel, EJ, Daniels, ER, Fairclough, DL & Clarridge, BR 1998, 'The practice of euthanasia and physician-assisted suicide in the United States: adherence to proposed safeguards and effects on physicians', JAMA, vol. 280, no. 6, pp. 507-513.
Emanuel, EJ, Fairclough, DL & Clarridge, BR 1996, 'Euthanasia and physician-assisted suicide: Attitudes and experiences of oncology patients, oncologists, and the public', Lancet, vol. 347, no. 9018, pp. 1805-1810.
Forde, R & Aasland, OG 2014, 'Are end-of-life practices in Norway in line with ethics and law?', Acta Anaesthesiol Scand, Aug 14.
Forde, R, Aasland, OG & Falkum, E 1997, 'The ethics of euthanasia -- attitude and practice maong Norwegian physicians', Social Science & Medicine, vol. 45, no. 6, pp. 887-982.
Gastmans, C, Lemiengre, J, van der Wal, G, Schotsmans, P & Dierckx de Casterle, B 2006, 'Prevalence and content of written ethics policies on euthanasia in Catholic healthcare institutions in Belgium (Flanders)', Health Policy, vol. 76, no. 2, pp. 169-78.
Imran, N, Haider, II, Jawaid, M & Mazhar, N 2014, 'Health ethics education: Knowledge, attitudes and practice of healthcare ethics among interns and residents in Pakistan', Journal of Postgraduate Medical Institute, vol. 28, no. 4, pp. 383-389.
Kuhse, H & Singer, P 1993, 'Voluntary euthanasia and the nurse: an Australian survey', International Journal of Nursing Studies, vol. 30, no. 4, pp. 311-322.
Kuhse, H, Singer, P, Baume, P, Clark, M & Rickard, M 1997, 'End-of-life decisions in Australian medical practice', Medical Journal of Australia, vol. 166, no. 4, pp. 191-196.
Lachman, V 2010, 'Physician-assisted suicide: compassionate liberation or murder?', Medsurg nursing : official journal of the Academy of Medical-Surgical Nurses, vol. 19, no. 2, pp. 121-125.
Malpas, P, Mitchell, K & Koschwanez, H 2015, 'End-of-life medical decision making in general practice in New Zealand—13 years on', New Zealand Medical Journal, vol. 128, no. 1418, pp. 27-39.
McGlade, KJ, Slaney, L, Bunting, BP & Gallagher, AG 2000, 'Voluntary euthanasia in Northern Ireland: General practitioners' beliefs, experiences, and actions', British Journal of General Practice, vol. 50, no. 459, pp. 794-797.
Mitchell, K & Owens, G 2004, 'End of life decision-making by New Zealand general practitioners: A national survey', New Zealand Medical Journal, vol. 117, no. 1196, pp. 1-11.
Muller, MT, Kimsma, GK & Van Der Wal, G 1998, 'Euthanasia and assisted suicide: Facts, figures and fancies with special regard to old age', Drugs and Aging, vol. 13, no. 3, pp. 185-191.
Nelson, B 1995, 'Euthanasia a family affair says top doc', The Sunday Territorian, Darwin, 21 May.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Riou, F, Aubry, R, Pontone, S & Pennec, S 2015, 'When physicians report having used medical drugs to deliberately end a patient's life: Findings of the "end-of-life in France" survey', Journal of Pain and Symptom Management, vol. 50, no. 2, pp. 208-215.
Rosenfeld, B 2000, 'Assisted suicide, depression, and the right to die', Psychology, Public Policy, and Law, vol. 6, no. 2, pp. 467-488.
Schwarz, JK 2003, 'Understanding and responding to patients' requests for assistance in dying', Journal of Nursing Scholarship, vol. 35, no. 4, pp. 377-384.
Schwarz, JK 2004, 'Responding to persistent requests for assistance in dying: a phenomenological inquiry', International Journal of Palliative Nursing, vol. 10, no. 5, pp. 225-235.
Seale, C 2009a, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, vol. 23, no. 3, pp. 198-204.
Seale, C 2009b, 'Hastening death in end-of-life care: a survey of doctors', Social Science & Medicine, vol. 69, no. 11, pp. 1659-1666.
Smith, SW 2007, 'Some realism about end of life: The current prohibition and the euthanasia underground', American Journal of Law and Medicine, vol. 33, no. 1, pp. 55-95.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, vol. 362, no. 9381, pp. 345-350.
Voultsos, P, Njau, SN & Vlachou, M 2010, 'The issue of euthanasia in Greece from a legal viewpoint', J Forensic Leg Med, vol. 17, no. 3, pp. 131-6.
Blog by Neil FrancisPosted on Saturday 2nd January 2016 at 12:35am
Dr William Toffler (left) acknowledges no slippery slope cause-and-effect evidence, with Drs Bentz and Stevens
A new scholarly journal focused on end-of-life ethics, decision-making and practice has just been launched: the Journal of Assisted Dying. In the first article, claims by Oregon lobby group Physicians for Compassionate Care (PCC), including Doctors Bill (William) Toffler and Ken Stevens (and others) are assessed against empirical evidence and found to be completely wrong, or highly misleading as a result of selective use of data.
The new scholarly journal, the Journal of Assisted Dying, is dedicated to careful and holistic analysis of evidence in regard to the various forms of assisted dying that are lawful in a number of jurisdictions around the world... and to practices in jurisdictions where assisted dying remains illegal.
In the first article of a series on Oregon, I examine claims and speculations made by various doctors (and others who quote them), that Oregon has the second-highest suicide rate in the USA (or is always in the top 10), that Oregon's Death With Dignity Act has resulted a massive increase in the state's general suicide rate, and other astonishing statements.
Of course, the empirical evidence from the Oregon Health Authority and from the USA Centers for Disease Control and Prevention does not support these statements and interpretations, and I analyse and critique the evidence.
Some of the claims are just plain factually and hugely wrong. Others are the result of failing to read their sources more carefully, misunderstanding what the data actually represents. Still further claims are made on the basis of selectively-chosen statements from government reports, while omitting statements that are contrary to, or provide alternative and well-researched explanations for Oregon's recently rising general suicide rate.
Drs Toffler and Stevens have even published some of their claims and speculations in the British Medical Journal.1 It goes to show that even good journals sometimes publish bunkum: their article was a letter to the editor rather than peer-reviewed research. Great care is required to sort real evidence from hype and opinion.
Ultimately, Dr Bill Toffler of PCC has acknowledged on video that there is no cause-and-effect evidence between Oregon's Death With Dignity Act and Oregon's suicide rate, an acknowledgement that went unchallenged by his two PCC colleagues present at the time, Dr Ken Stevens and Dr Chuck (Charles) Bentz. You can see Dr Toffler's statement here (at 10'50").
The Journal of Assisted Dying is an open-access journal, and you can read the full article here.
-----
1. Toffler, WL & Stevens, K 2015, 'Re: Assisted dying: law and practice around the world', BMJ, vol. 351, 19 Aug, p. h4481.
Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 1–6.
Abstract
Background: Several physicians have speculated that Oregon’s general suicide rate is evidence of suicide contagion as a result of Oregon’s Death With Dignity Act (‘the Act’). Methods: Search and analysis of physician and related online sources of Oregon suicide contagion speculation; retrieval and analysis of cited Centers for Disease Control and Prevention (CDC) and other publications relied upon; analysis of authoritative, public Government mortality data for Oregon and other USA states. Results: Several physicians have speculated about Oregon suicide statistics in a manner that is not supported by the cited publications, or by public CDC mortality database data. The claims variously (a) misrepresent key data in the publications, (b) omit information in the publications that is at variance with suicide contagion speculation, and (c) overlook other significant information at variance with speculation. The physicians have previously acknowledged inability to prove perceived “slippery slope” effects of the Act. Other opponents of the Act have republished the physicians’ erroneous information. Conclusions: Evidence advanced by several physicians to speculate that Oregon’s Death With Dignity Act causes suicide contagion in Oregon is variously false, misleading or highly selective—omitting key facts—and has arisen even though the physicians acknowledge they have no proof of ‘slippery slope’ effects.
Article keywords
suicide contagion, copycat suicide, Werther effect, slippery slope, misinformation, Oregon, Dr William Toffler, Dr Kenneth Stevens, Physicians for Compassionate Care
Full PDF
Download the full PDF: (390Kb)
Citation
Francis, N 2016, 'Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon', Journal of Assisted Dying, vol. 1, no. 1, pp. 1-6.
Blog by Neil FrancisPosted on Sunday 22nd November 2015 at 5:05am
The Parliament of Victoria is conducting an inquiry into end-of-life decision making.
The standing Legal and Social Issues Comittee of the Parliament of Victoria, Australia, is currently conducting an inquiry into end-of-life decision making, to inform any legislative changes required in order to reflect contemprary views and best practice.
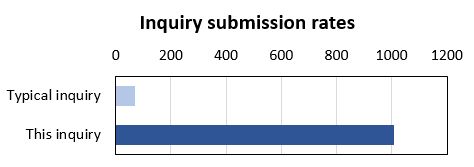
The inquiry has certainly engaged the community: it has received a record number of submissions. The Legal and Social Issues Committee typically receives a couple of dozen submissions to any of its inquiries, occasionally even sixty or eighty. In contrast, the inquiry on end-of-life decision making has received more than one thousand (1,017) submissions.
Most of the submissions (98%), including DyingForChoice.com's, are published on the Committee's website, with the tiny remainder kept confidential at the request of the submitter.
The terms of reference for the inquiry are completely silent on the matter of assisted dying. The Terms talk about "making informed decisions", "exercising preferences" and "the role of palliative care" in the context of current legislation and any required changes.
So, given that assisted dying is not mentioned in the Terms of Reference, you'd expect a modest number of submissions to address the issue, right? Wrong.
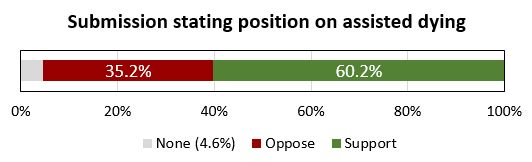
Of the submissions that are published on the Committee's website (and which I could therefore read), a staggering 95.4% of them make specific and deliberate points about assisted dying law reform, and 60.2% of the published submissions make points in favour of law reform to permit assisted dying in one form or another.
There is no clearer indication than this of how deeply engaged the Victorian public is with end-of-life decision making, and how important assisted dying law reform is to the options they might consider.
The Leglislative Council and this Committee are to be highly commended for establishing and conducting the inquiry. Public hearings with witness appearances have further helped inform the Committee and its Secretariat. The transcript of my appearance can be read here.
We the people of Victoria look forward with anticipation to the final report of the Committee, and the recommendations it makes. The Committee must report back to the Legislative Council no later than 31st May 2016. But, given the tsunami of submissions and the continuing public hearings, we won't be surprised if the Committee is granted an extension to complete its work.
Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
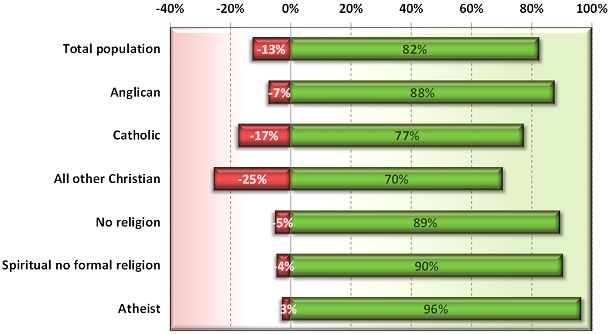
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
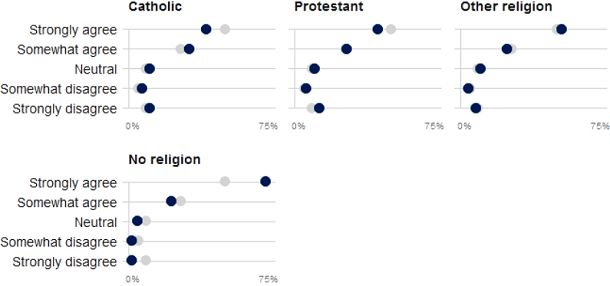
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
Blog by Neil FrancisPosted on Thursday 23rd July 2015 at 1:22am
The Victorian Premier doesn't support assisted dying law reform - at this stage.
Victorian Premier Daniel Andrews reports that he doesn’t support voluntary euthanasia “at this stage” (The Age, 21 Jun 2015), and that his objections are not based on his Catholic faith. I think it is fair to take him at his word given his historical record in facilitating conversation and reform around values-based issues such as abortion. But his current thinking on assisted dying is indefensible as I explain.
We know from repeated Newspoll Australia studies that amongst the millions of Victorians who want the State to respect their wish to make their own choices at the end of life, three out of four Australian Catholics are in favour of legalised assisted dying—at odds with the ‘traditional’ Catholic stance. Mr Andrews, like a majority of Catholic Australians, may simply not agree with the Vatican line on assisted dying choice, as they don't on a range of matters.
Mr Andrews says that his current objections instead revolve around ‘safeguard’ and ‘balance’ issues in a context of finite healthcare resources.
The Medical Treatment Act 1988 confers the right to Victorian patients to refuse any medical treatment. The right applies even if the treatment is life-saving, for example a simple blood transfusion. The Act contains no ‘safeguards’, as the Premier refers to them:
The patient is not required to give any reason;
The doctor is not required to inform the patient of their condition or likely consequences of any treatment or its refusal;
The doctor is not required to consider or assess the patient’s mental capacity to decide including depression;
The doctor is not required to recommend a palliative consult (if relevant);
The doctor is not required to consult any colleagues for a further opinion about the patient’s illness or mental capacity;
There is no obligation on the patient to consider their decision again after a short time;
While there is a standard form 'Refusal of Medical Treatment' document that can be signed to provide documentary evidence of the refusal, it is not mandatory;
There is no mandated path of reporting or review.
Indeed, a doctor who goes on to administer medical interventions to the patient who has refused them is guilty of the offence of ‘medical trespass’ and can be prosecuted.
Further, it is quite legal for a patient to decide to die by voluntary refusal of food and fluids, an option suggested as appropriate by Dr Bill Sylvester in an IQ2 debate at Melbourne Town Hall in November 2012, to a hostile reaction from the audience. Some doctors provide respite care to patients choosing this path. however, like refusal of medical treatment, there are no legislated safeguards.
On the basis of these two kinds of end-of-life decision making that have been lawful for at least a quarter century in Victoria, and which have no legislated safeguards, what evidence do we have of the so-called ‘slippery slope’ of resource-strapped healthcare providers or greedy relatives persuading the sick to choose a path to die earlier rather than later?
Both Victoria Police and the former Minister for Health, the Hon. David Davis, have advised that there are no known prosecutions under the provisions of the Medical Treatment Act 1988 for such inappropriate persuasion.
So, in Victoria we have the experience of two forms of decision-making whose direct and foreseeable consequence is death, with no mandated safeguards and within 'finite healthcare resources' (which Mr Andrews refers to as his reason), not resulting in prosecutions for persuasion to 'choose' death.
If Mr Andrews’ argument is that terminally ill Victorians ought to be denied the right to choose assisted dying because of supposed slippery slopes of persuasion, that argument would exactly and equally apply to the refusal of life-saving medical treatment and to the refusal of food and fluids.
Surely his Government is not suggesting that the existing rights be rescinded: that patients be forced to receive any and all life-saving and life-prolonging treatment in order to avoid a 'persuasion' bogeyman who doesn’t exist?
The Premier's stance is even less defensible in the light of proposed assisted dying legislation which includes a suite of checks and balances that are absent from existing rights.
Some dying individuals, reflecting upon their circumstances and deeply-held values and beliefs, determine that alighting from the train of terminal illness one or two stops before the terminus is a vastly better option than being forced to endure the train ride until the very end. We compound their indignities by saying it’s OK to decide to starve yourself to death (and we might even provide support along the way), but not OK to decide to die peacefully surrounded by loved ones at a predetermined time.
It is commendable that the Legislative Council has resolved to investigate the issue of end-of-life decisions, and whose final report will better inform the Premier and all Parliamentarians. Submissions to the Committee are open until Monday 31st August.
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:28pm
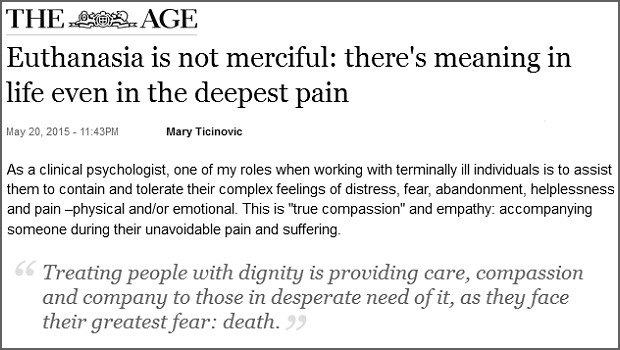
The opinion piece in The Age.
In today’s Fairfax press, Sydney woman Mary Ticinovic advances a number of reasons as to why she believes that assisted dying is not merciful. The by-line identifies her as a “clinical psychologist”. But her arguments are not founded on the basic tenets of psychology. How so?
Mary argues that to support assisted dying is to go “against the principle that all life is precious.” She offers no substantive explanation, invoking the notion of ‘human worth’, stating that it exists regardless of the health state or suffering of the person, and complaining that assisted dying promotes the idea that “your life is no longer worth living”.
These are not psychological arguments. We can agree that life is precious. But reluctantly deciding to hasten one’s death in the face of intolerable and unrelievable terminal suffering doesn’t negate that preciousness. Indeed, to some people, choosing assisted dying can evidence the preciousness of one’s very capacities and values as a human.
Whose standards?
Mary further muses over “by whose standards would we judge if life is not worthwhile any more”, as though this is only some vague theoretical argument amongst philosophers or doctors. This is not a psychological argument, either. Under assisted dying law reform, it is only the dying individual’s world-view and circumstances that determine whether he or she feels life is worth living: not anyone else. General philosophical theory doesn’t come into it.
She further argues that assisted dying “promotes a utilitarian view of humanity”. This is not a psychological argument, either. Nor is it valid. Indeed, legalised assisted dying respects the very nature of the diversity of humanity by enabling the world-views many people hold most dear: that of making rational choices consistent with their own beliefs, values and circumstances. Some patients, for example in Oregon, are deeply religious and believe that their God is compassionate and understands and respects their choice to avoid intolerable suffering. That’s not utilitarian at all.
Harm and the Hippocratic Oath
Mary invokes the Hippocratic Oath said by her medical friends to oblige doctors to “do no harm” and that the medical role is “in healing and helping the patient to be restored to health.” This is simplistic nonsense, not a psychological argument.
Firstly, doctors do harm all the time: think of surgical procedures or chemotherapy. Many medical interventions do harm, but we accept the harm because we expect there to be a commensurately greater good as a result.
Secondly, medical practice cannot always “restore the patient to health” as Mary exclusively puts it. What then? The dying patient may judge that the unrelievable suffering they will experience along the path to death is a greater harm than dying a little earlier. And, doctors also have a primary duty to relieve suffering, which Mary doesn’t mention. What is under review is whether a doctor may participate in the relief of intolerable and unrelievable suffering— by hastening death—if the patient believes this is the lesser harm.
Thirdly, the Hippocratic Oath is around 2,300 years old. It requires doctors to swear allegiance to ancient Greek gods. It forbids women from becoming doctors. It requires current doctors to train the next generation free of charge, and it forbids surgery. Contemporary doctors don’t take it, and it’s certainly not “part of training” as Mary mistakenly states.
None of these are psychology arguments.
'Sucker’s choice'
Mary then argues that requiring dying patients to endure until the end promotes—and that assisted dying prevents—“fostering gratitude”, “reconciling hurts or differences with family members or friends” and “showing them strategies or different ways to approach their pain and suffering”.
But, in jurisdictions where assisted dying is legal, for example in Oregon in the USA, these are precisely things that are encouraged under assisted dying. Doctors are required to inform applicants of available medical and palliative interventions. Family gathers on notice of an anticipated death, music and poetry is shared, and expressions of love, devotion and gratitude are exchanged.
If a dying patient has no intention of reconciling with family or reflecting on approaches to dealing with their pain and suffering under an assisted dying law, precisely the same intention applies to the current regime that requires the patient to endure until the end. To assume a difference is a false dichotomy.
Obligatory compassion
Mary also argues that assisted dying ought to remain outlawed because “nursing a sick loved one is a way to give back”. This is yet another specious non-psychology argument. It promotes the ‘right’ of the ‘nurse’ to express love and devotion through ‘caring interventions’ at the expense of the dying patient’s own world view and deeply-held wish for a hastened death. Now who’s being utilitarian?
The upshot
I ran Mary’s opinion piece past an experienced psychologist, who described it as little to do with psychology. Note that neither of us has experience of or is commenting on Mary’s expertise as a clinical psychologist: she may indeed be a very good one.
My associate wondered out loud if Mary’s arguments were based more on underlying religious views than anything else. I agreed: they seemed to me remarkably consistent with the arguments advanced by religious opponents, even though they avoided directly religious words. So I did a little research.
It turns out that Mary is a committed and active Sydney Catholic.* Evidence abounds of her devotion to the Catholic tradition, and I commend her for her conscientious reflective practice and participation in it.
However, I argue that neither the stated psychological qualification nor the unstated religious affiliation make the offered arguments valid.
-----
* By way of fairness, I place on the record that I am agnostic.
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:06pm
Neil Francis announces the official launch of DyingForChoice.com, the world's premier source of reliable, evidence-based information about assisted dying, and responsible law reform to permit it in restricted circumstances.
Hi, and thanks for dropping by.
I'm delighted to announce the official launch of DyingForChoice.com. The mission is to help society work towards responsible assisted dying law reform, a reform wanted by the great majority of citizens in many countries. Yet assisted dying (in one form or another) is still illegal in many jurisdictions.
DyingForChoice.com will lay out the case for restricted assisted dying including world-view arguments, but also importantly provide rigorous factual evidence and analysis. This approach is a deliberate counter-measure to mistaken information — 'misinformation', more colloquially known as 'bull' — that is available so widely and repeated so often.
Misinformation can take the form of flapdoodle, filibuster, flip-flop, fudge or outright fiction. Ultimately it's fear-mongering via the promotion of bull. Legislative reform — so that all citizens are afforded the right to enact their own deeply-held world views and cherished values at the end of life, whatever those may be — deserves to be informed by quality information.
Exposing misinformation works. Already, my exposure of the 'suicide contagion' myth has resulted in selected website 'information' being withdrawn. It's up to all of us to hold a bright spotlight up to misinformation and to ask people not to spread bull.
So subscribe to our monthly newsletter to keep abreast of developments. You can also create your own login which will allow you to comment on posts, subject of course to our terms of use. Just use the Register link in the header bar.
You can also subscribe to our Twitter feed, catch up with our Facebook page, and watch any of our videos on our YouTube channel: just click the relevant button in the header bar.
So, keep in touch, stay up to date, and if you have a burning issue you would particularly like us to report on, just send a message using our Contact form.
 Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.