Blog by Neil FrancisPosted on Sunday 28th August 2016 at 12:58am
Brad Mattes' blog containing misleading and evidentially false statements.
The latest misinformation employed by assisted dying opponents is to imply that Belgium’s general suicide rate is high as a consequence of its assisted dying law: i.e. to argue the discredited 'suicide contagion' line which has in the past been peddled about the USA state of Oregon. I have demonstrated that it was false in Oregon, and I equally demonstrate here that it's false in Belgium.
Mr Brad Mattes recently published emotional anti-assisted-dying nonsense in LifeSiteNews. (LifeSiteNews is a Canadian blog site that was established by the conservative Christian Campaign for Life Coalition and which has a primary principle of promoting “traditional Judeo-Christian principles”. Mr Mattes is radio host for Ohio’s Life Issues Institute, an anti-abortion lobby group established by conservative American John C. Willke who claimed that women’s bodies were resistant to pregnancy as a result of rape.)
Putting on the misinformation running shoes
In his blog Mr Mattes quickly establishes a practice of communicating misinformation by first claiming that assisted dying laws have “devastating effects” around the world including Japan and Albania—which don’t have such laws.
He then sprints onwards to the ‘650 babies euthanized in the Netherlands’ claim—which I have already comprehensively exposed as fake in the Journal of Assisted Dying—and then onto the bogus claim that the Netherlands has descended into a mire of ‘killing’ without the patient’s ‘consent,’ contrary to empirical evidence I've published that such actions occur around the world regardless of assisted dying laws, and which have decreased significantly in the Netherlands and Belgium since their assisted dying statutes came into effect in 2002.
Let’s add fries to that
Having served up a lot of fat and salt that might appeal to those on a fast-food anti-assisted-dying diet, he then offers the unqualified statement:
“By the way, Belgium has the second-highest suicide rate (nonrelated to euthanasia) in Western Europe.” — Brad Mattes
The ‘informational’ consequence is unequivocal: by Mr Mattes failing to contextualise this ‘incidental factoid’ in any way, the reader is destined to deduce that it is Belgium’s euthanasia law that causes Belgium’s suicide rate to be the second-highest in Western Europe. In other words, Mr Mattes is another poorly-informed commentator using the 'suicide contagion' line.
But what are the facts?
Depending on the source and year of data, one can certainly argue that Belgium’s general suicide rate is the second-highest in Western Europe. Setting aside for now the serious question of why it is valid to exclude all of the world’s other countries from the comparison, WorldLifeExpectancy.com reports figures that were published in 2014 (Table 1).
Table 1
Country
Suicides*
Finland
15.11
Belgium
14.64
Iceland
14.06
France
12.84
Austria
11.87
Sweden
11.43
Ireland
11.06
Germany
9.59
Switzerland
9.56
Norway
9.28
Denmark
9.19
Luxembourg
9.14
Netherlands
8.54
Portugal
8.49
Turkey
7.92
UK
6.28
Malta
5.75
Spain
5.23
Italy
4.76
Greece
3.86
* Suicides per 100k population, age-adjusted
The table includes all the countries in the wider definition of “Western Europe”, bar four: no suicide statistics are published for Liechtenstein, Monaco, Andorra or San Marino.
As you can see, Belgium is indeed the second-highest. But this begs the question:
If the reason Belgium is the second-highest is due to its assisted dying law, how come Finland, which Mr Mattes doesn't mention by name and which has no such law, is higher?
It also begs the question:
If assisted dying law were the fundamental cause of a high general suicide rate, how come Switzerland (statute since 1942), Luxembourg (statute since 2009) and the Netherlands (practice since the early 1980s and statute since 2002) have rates that are muchlower, all key facts that Mr Mattes also fails to mention?
These are of course indications that the factoid has been included as a cherry-picked morsel of 'proof' because it sounds so compelling as a throw-away sentence amongst the other (false) statements.
But wait, there’s more
We can go further than merely wondering about the country comparisons, by comparing Belgium’s general suicide rate before and after assisted dying law reform. A critical step in establishing causation is to first establish correlation. If there is no correlation, there can be no causation.
Published OECD data shows that in 2013 (the most recent available data), Belgium’s general suicide rate was 16.7 per 100,000 population. What was it before their 2002 law reform? Well in 2000 it was 20.5, in 1990 it was 19.2, … you get the idea.
Has Belgium’s general suicide rate soared (or even increased modestly) since their 2002 assisted dying law came into effect? No. It’s dropped. Indeed, the slight downward trend apparent before the statute came into effect in 2002 has accelerated downward since (Figure 1).
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Even the headline is misleading
Mr Mattes fails to point out in his blog that assisted dying statutes in Benelux countries (Belgium, the Netherlands and Luxembourg) never restricted access to only the 'terminally ill,' that is, those imminently dying. He also fails to point out that USA states whose laws do restrict assisted dying to the terminally ill—most notably Oregon and Washington—have not changed their statutes in this regard since they came into effect.
Therefore, his headling implying that lawful jurisdictions have broadened their laws from 'only the terminally ill' is also wrong.
Conclusion
Mr Mattes makes multiple false and misleading claims and it’s easy to see his opinion for what it is: an emotional dump that fails to engage with and indeed flies in the face of actual evidence. The latest 'suicide contagion' implication, that assisted dying law causes Belgium’s general suicide rate to be the “second-highest in Western Europe” is evidentially false.
I call on LifeSiteNews to withdraw Mr Mattes' article because it breaches their primary principle:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.” — LifeSiteNews
Summary of facts
Belgium's general suicide rate is one of the higher ones in Western Europe. However:
At least one country without an assisted dying law has a higher suicide rate, inconsistent with 'suicide contagion' theory.
Other Western Europe countries with assisted dying laws have suicide rates much lower than Belgium's, also at odds with 'suicide contagion' theory.
But the clincher is that the suicide rate in Belgium has dropped, not risen, since their 2002 assisted dying law came into effect.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
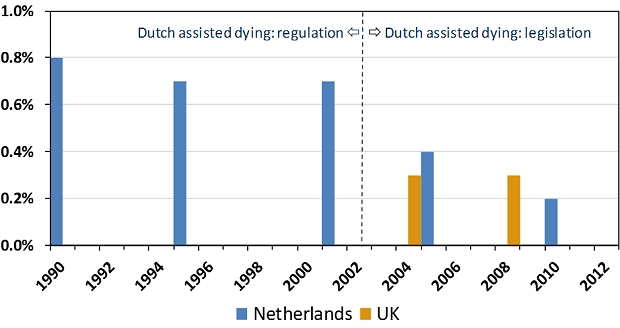
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.
Fact file by Neil FrancisPosted on Thursday 28th January 2016 at 1:30am
Around the world, doctors help patients with assisted dying, regardless of whether it is legal in their jurisdiction or not.
For example, in Australia, where assisted dying is illegal, research reveals that assisted dying is widely practiced. Many Australian nurses have collaborated with doctors to provide assisted dying, and have occasionally even done so without consulting a doctor (Kuhse & Singer 1993). Nurses in New Zealand also provide assisted dying, sometimes without consulting a doctor (Malpas, Mitchell & Koschwanez 2015; Mitchell & Owens 2004).
"Euthanasia is common. It's practiced out of sight, under wraps, no regulation, no rules, no supervision." Prof. Peter Baum (Baum 2001)
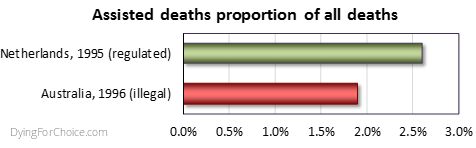
Professor Baum's statement is borne out by scientific research. A national survey of Australian doctors in 1996 found that 1.9% of deaths were the result of voluntary euthanasia (VE) or physician-assisted dying (PAD) (Kuhse et al. 1997). By comparison, the rate in the Netherlands in 1995 (the closest year of empirical research data) was 2.6% (Onwuteaka-Philipsen et al 2012). The rate of medically assisted deaths in Australia, where the practice is illegal, was three quarters the rate of the Netherlands, where the practice is legal.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Forms of medically assisted dying have been found to occur not only in Australia (and in the Netherlands where it has been lawful for decades), but in Belgium prior to its law reform (Chambaere et al. 2015); Switzerland, Denmark, Sweden and Italy (van der Heide et al. 2003); the UK (Seale 2009a; Seale 2009b); the USA (Back et al. 1996; Bonn 2000; Emanuel, Fairclough & Clarridge 1996; Lachman 2010; Schwarz 2003; Schwarz 2004); France (Riou et al. 2015); Norway (Forde & Aasland 2014; Forde, Aasland & Falkum 1997); and even in conservative Greece (Voultsos, Njau & Vlachou 2010); Northern Ireland (McGlade 2000) and Pakistan (Imran et al. 2014).
Indeed, "euthanasia is performed worldwide, regardless of the existence of laws governing it" (Gastmans et al. 2006), "in all countries studied" (Muller, Kimsma & Van Der Wal 1998), "albeit in a secretive manner" (Rosenfeld 2000), "in the privacy of their [doctor-patient] relationship" (Cassell 1995), with repeated involvement of some physicians (Smith 2007), and frequent failure to adhere to high standards when illegal (Emanuel et al 1998).
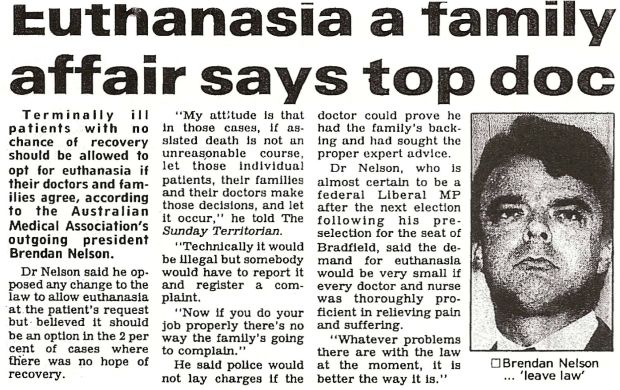
Even Dr Brendan Nelson, while President of the Australian Medical Association, acknowledged that he had helped hasten the death of a patient. He stated that in the "2 percent of cases" where there was no hope of recovery, that "patients, their families and their doctors make those decisions [for euthanasia]" though clandestinely, because "technically it would be illegal" (Nelson 1995).
AMA's President, Brendan Nelson, in 1995.
The evidence is irrefutable: there is underground assisted dying worldwide and it demonstrates that there is a profound need for assisted dying law reform to allow dying patients the right to seek a peaceful hastened death, and to protect doctors and nurses who provide that assistance. Law reform would also force assisted dying from the dark shadows, creating transparency and accountability around the process, which would then be open to discussion and improvement if required.
Intolerable and unrelievable patient suffering drives underground assisted dying across the world in jurisdictions where it is illegal, with no standards of practice or transparent oversight.
References
Back, AL, Wallace, JI, Starks, HE & Pearlman, RA 1996, 'Physician-assisted suicide and euthanasia in Washington State: Patient requests and physician responses', JAMA, vol. 275, no. 12, pp. 919-925.
Baum, P 2001, ABC News, TV broadcast 23 Jan, ABC, Sydney.
Bonn, D 2000, 'Support for euthanasia falls as care of dying patients improves', The Lancet Oncology, vol. 1, no. 3, p. 133.
Cassell, EJ 1995, 'Treating the patient's subjective state', Pain Forum, vol. 4, no. 3, pp. 186-188.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, vol. 372, no. 12, pp. 1179-1181.
Douglas, C, Kerridge, IH, Rainbird, KJ, McPhee, JR, Hancock, L & Spigelman, AD 2001, 'The intention to hasten death: a survey of attitudes and practices of surgeons in Australia', Medical Journal of Australia, vol. 175, no. 10, pp. 511-515.
Emanuel, EJ, Daniels, ER, Fairclough, DL & Clarridge, BR 1998, 'The practice of euthanasia and physician-assisted suicide in the United States: adherence to proposed safeguards and effects on physicians', JAMA, vol. 280, no. 6, pp. 507-513.
Emanuel, EJ, Fairclough, DL & Clarridge, BR 1996, 'Euthanasia and physician-assisted suicide: Attitudes and experiences of oncology patients, oncologists, and the public', Lancet, vol. 347, no. 9018, pp. 1805-1810.
Forde, R & Aasland, OG 2014, 'Are end-of-life practices in Norway in line with ethics and law?', Acta Anaesthesiol Scand, Aug 14.
Forde, R, Aasland, OG & Falkum, E 1997, 'The ethics of euthanasia -- attitude and practice maong Norwegian physicians', Social Science & Medicine, vol. 45, no. 6, pp. 887-982.
Gastmans, C, Lemiengre, J, van der Wal, G, Schotsmans, P & Dierckx de Casterle, B 2006, 'Prevalence and content of written ethics policies on euthanasia in Catholic healthcare institutions in Belgium (Flanders)', Health Policy, vol. 76, no. 2, pp. 169-78.
Imran, N, Haider, II, Jawaid, M & Mazhar, N 2014, 'Health ethics education: Knowledge, attitudes and practice of healthcare ethics among interns and residents in Pakistan', Journal of Postgraduate Medical Institute, vol. 28, no. 4, pp. 383-389.
Kuhse, H & Singer, P 1993, 'Voluntary euthanasia and the nurse: an Australian survey', International Journal of Nursing Studies, vol. 30, no. 4, pp. 311-322.
Kuhse, H, Singer, P, Baume, P, Clark, M & Rickard, M 1997, 'End-of-life decisions in Australian medical practice', Medical Journal of Australia, vol. 166, no. 4, pp. 191-196.
Lachman, V 2010, 'Physician-assisted suicide: compassionate liberation or murder?', Medsurg nursing : official journal of the Academy of Medical-Surgical Nurses, vol. 19, no. 2, pp. 121-125.
Malpas, P, Mitchell, K & Koschwanez, H 2015, 'End-of-life medical decision making in general practice in New Zealand—13 years on', New Zealand Medical Journal, vol. 128, no. 1418, pp. 27-39.
McGlade, KJ, Slaney, L, Bunting, BP & Gallagher, AG 2000, 'Voluntary euthanasia in Northern Ireland: General practitioners' beliefs, experiences, and actions', British Journal of General Practice, vol. 50, no. 459, pp. 794-797.
Mitchell, K & Owens, G 2004, 'End of life decision-making by New Zealand general practitioners: A national survey', New Zealand Medical Journal, vol. 117, no. 1196, pp. 1-11.
Muller, MT, Kimsma, GK & Van Der Wal, G 1998, 'Euthanasia and assisted suicide: Facts, figures and fancies with special regard to old age', Drugs and Aging, vol. 13, no. 3, pp. 185-191.
Nelson, B 1995, 'Euthanasia a family affair says top doc', The Sunday Territorian, Darwin, 21 May.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Riou, F, Aubry, R, Pontone, S & Pennec, S 2015, 'When physicians report having used medical drugs to deliberately end a patient's life: Findings of the "end-of-life in France" survey', Journal of Pain and Symptom Management, vol. 50, no. 2, pp. 208-215.
Rosenfeld, B 2000, 'Assisted suicide, depression, and the right to die', Psychology, Public Policy, and Law, vol. 6, no. 2, pp. 467-488.
Schwarz, JK 2003, 'Understanding and responding to patients' requests for assistance in dying', Journal of Nursing Scholarship, vol. 35, no. 4, pp. 377-384.
Schwarz, JK 2004, 'Responding to persistent requests for assistance in dying: a phenomenological inquiry', International Journal of Palliative Nursing, vol. 10, no. 5, pp. 225-235.
Seale, C 2009a, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, vol. 23, no. 3, pp. 198-204.
Seale, C 2009b, 'Hastening death in end-of-life care: a survey of doctors', Social Science & Medicine, vol. 69, no. 11, pp. 1659-1666.
Smith, SW 2007, 'Some realism about end of life: The current prohibition and the euthanasia underground', American Journal of Law and Medicine, vol. 33, no. 1, pp. 55-95.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, vol. 362, no. 9381, pp. 345-350.
Voultsos, P, Njau, SN & Vlachou, M 2010, 'The issue of euthanasia in Greece from a legal viewpoint', J Forensic Leg Med, vol. 17, no. 3, pp. 131-6.
Blog by Neil FrancisPosted on Sunday 22nd November 2015 at 5:05am
The Parliament of Victoria is conducting an inquiry into end-of-life decision making.
The standing Legal and Social Issues Comittee of the Parliament of Victoria, Australia, is currently conducting an inquiry into end-of-life decision making, to inform any legislative changes required in order to reflect contemprary views and best practice.
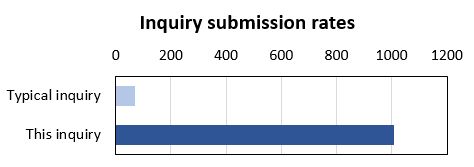
The inquiry has certainly engaged the community: it has received a record number of submissions. The Legal and Social Issues Committee typically receives a couple of dozen submissions to any of its inquiries, occasionally even sixty or eighty. In contrast, the inquiry on end-of-life decision making has received more than one thousand (1,017) submissions.
Most of the submissions (98%), including DyingForChoice.com's, are published on the Committee's website, with the tiny remainder kept confidential at the request of the submitter.
The terms of reference for the inquiry are completely silent on the matter of assisted dying. The Terms talk about "making informed decisions", "exercising preferences" and "the role of palliative care" in the context of current legislation and any required changes.
So, given that assisted dying is not mentioned in the Terms of Reference, you'd expect a modest number of submissions to address the issue, right? Wrong.
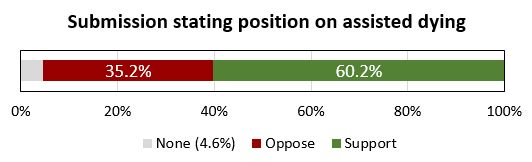
Of the submissions that are published on the Committee's website (and which I could therefore read), a staggering 95.4% of them make specific and deliberate points about assisted dying law reform, and 60.2% of the published submissions make points in favour of law reform to permit assisted dying in one form or another.
There is no clearer indication than this of how deeply engaged the Victorian public is with end-of-life decision making, and how important assisted dying law reform is to the options they might consider.
The Leglislative Council and this Committee are to be highly commended for establishing and conducting the inquiry. Public hearings with witness appearances have further helped inform the Committee and its Secretariat. The transcript of my appearance can be read here.
We the people of Victoria look forward with anticipation to the final report of the Committee, and the recommendations it makes. The Committee must report back to the Legislative Council no later than 31st May 2016. But, given the tsunami of submissions and the continuing public hearings, we won't be surprised if the Committee is granted an extension to complete its work.
Blog by Neil FrancisPosted on Sunday 15th November 2015 at 2:38am
ABC TV's Q&A panel discusses assisted dying law reform on 9th Nov 2015
In a recent opinion piece in the ABC’s Religion and Ethics section, Bernadette Tobin1 rails against assisted dying, commencing with the criticism that the ABC’s Q&A discussion on the subject this week “lacked precision.” But Tobin’s opinion piece itself commits exactly this offence, as I explain.
For the sake of brevity I’ll only quickly mention that Tobin’s piece also fails on the score of accuracy. For example, she wrongly asserts that “euthanasia” means a doctor administering lethal medication to a patient. It doesn’t. “Euthanasia” simply means “good death”: nothing more and nothing less, regardless of how it occurs. Tobin also asserts that voluntary euthanasia in lawful jurisdictions has caused non-voluntary euthanasia to develop. This is the polar opposite of published empirical research evidence.
But back to precision. Tobin employs two imprecise and deeply flawed arguments in her objection to assisted dying. She variously rolls them in together, so let’s unpack what they are: (A) the “it’s only fair” slippery slope, and (B) “it’s OK if you don’t mean it”.
A: The “It’s only fair” slippery slope
Tobin directly links assisted dying for the terminally ill to “anyone who is in pain, discomfort, constipated, incontinent, depressed, anxious and so on” by way of potential “benefit”. She conjectures that increasing the restrictions to who may qualify, and the process of qualification, would then be “unfair” to these others. She then goes on to extend the argument to those lacking in decisional capacity such as infants and those with Alzheimer’s. Surely, she says, “it would be ‘unfair’ to deny these people the ‘benefit’ that we will make available to those who are able to request it?”
Slippery slope indeed. And it’s wrong. Let me illustrate how, using a topic familiar in political debate over recent years: same-sex marriage.
Opponents of same-sex marriage law reform, when using arguments of the kind Tobin offers (as they often do), say that we can’t allow two men to marry, or two women to marry, because then we would have to allow three or more people to marry. Further down the slippery slope, we would have to allow people to marry animals. Don’t laugh: such things have been argued.
Next—given that under the Corporations Act 2001 (Cth), companies, owners’ corporations and incorporated associations are at law ‘persons’, and now that persons may marry—it would be “unfair” (note that I’ve used imprecision quotation marks around the word as Tobin does) to disallow people from marrying companies and companies from marrying each other.
Finally, using Tobin’s own line of argument, it would be “unfair” to deny infants and those with Alzheimer’s being married off for the alleged “benefit” (those quotation marks again) that everyone else is enjoying, so we must as an unavoidable consequence of the first step of allowing same-sex marriage, allow arranged marriages for babies and those with advanced dementia.
By now it’s easy to spot two terminal flaws in Tobin’s argument.
Firstly, the use of just one criterion (“fairness”—which she leaves imprecisely undefined) as the sole basis for decision making about this legislative reform is indefensible. What about other critical factors such as well-informed, rational, decisional capacity, judging and weighing what a “benefit” is, in the face of intolerable and unrelievable suffering, consistent with one’s own values and beliefs, who may decide, and the right not to participate?
Secondly, any slippery slope’s purported summit (from which changes are argued only to slip downwards) is deeply rooted in the normativity of the present. We are used to marriage being between a man and a woman. In our relative comfort we accept it as ‘normal,’ ‘good’ and the ‘right thing’.
In decision-making scholarship this normativity is known as “anchoring”. Like an anchor around which a boat will swing according to the wind and tide, we take the pivot point (the anchor of the now), as the natural starting point for future decisions, comparing changes only to the present state of affairs.
But it isn’t a valid anchor, and assuming that it is seriously biases our thinking. We need cast our anchor back just one mooring from the current point to see how the anchor tints our decision-making spectacles:
“We can’t allow a man and a woman to marry, because then it would be unfair to not allow two men to marry, or two women to marry, and then…”
Clearly, it is imperative that we outlaw marriage altogether.
The upshot of this slippery slope, when followed properly to its own logical conclusions, is that we must deny all rights because we can confect a slippery slope into a hypothetical moral abyss for any right.
B: It’s OK if you don’t mean it
Tobin further argues that relieving distressing symptoms “is good palliative care, even when that relief happens to hasten death.”
She doesn’t name it explicitly, but this is the doctrine of double effect, an argument first crafted in the thirteenth century by Catholic priest Thomas Aquinas. The doctrine suggests that a bad consequence of an action is justifiable if the agent did not intend the bad effect, if the intended good effect outweighs the bad effect, and if the agent applies diligence in attempting to minimise the bad effect. Notice that the doctrine speaks directly about the intentions of the agent and is silent on the views of the person upon whom the agent might act.
Tobin rails against a doctor intentionally administering a lethal dose to a patient (regardless of whether it is the dying patient’s most fervent wish) and slams the expressions “dying with dignity” and “aid in dying” as “fudges”.
Yet the doctrine of double effect, for which she argues in support, is itself a fudge because it says:
“It’s OK to for a doctor to decide to and actually kill their patient (after all, they hastened the patient’s death), as long as they don’t mean to, and they mean well.”
What kind of standard is the secret stuff that goes on inside a doctor’s head without reference of any kind to the patient’s own views and desires, when compared to a fully informed, documented and tested request from the patient?
It’s no wonder that many scholars (as do I) consider the doctrine of double effect problematic.
--
Bernadette Tobin is the Director of the Plunkett Centre for Ethics, a joint initiative of St Vincent’s Hospital, Sydney, and Australian Catholic University (ACU). According to ACU, a core mission of the Centre is to “bring a Catholic perspective to all its endeavours”.2
It’s unsurprising then that I detected neither broad thrust nor any detail of Tobin’s ABC opinion piece that deviated from the views of the Vatican. So be it.
There are many points on which Tobin and I agree, such as the potential benefits of palliative care for the dying. I argue, though, that basic scrutiny of the proffered 'principles' reveal them as deeply flawed and unpersuasive.
Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
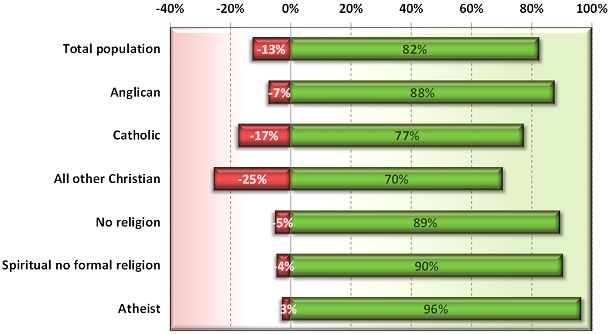
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
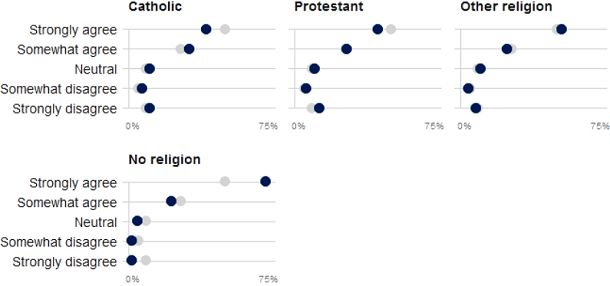
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:28pm
The opinion piece in The Age.
In today’s Fairfax press, Sydney woman Mary Ticinovic advances a number of reasons as to why she believes that assisted dying is not merciful. The by-line identifies her as a “clinical psychologist”. But her arguments are not founded on the basic tenets of psychology. How so?
Mary argues that to support assisted dying is to go “against the principle that all life is precious.” She offers no substantive explanation, invoking the notion of ‘human worth’, stating that it exists regardless of the health state or suffering of the person, and complaining that assisted dying promotes the idea that “your life is no longer worth living”.
These are not psychological arguments. We can agree that life is precious. But reluctantly deciding to hasten one’s death in the face of intolerable and unrelievable terminal suffering doesn’t negate that preciousness. Indeed, to some people, choosing assisted dying can evidence the preciousness of one’s very capacities and values as a human.
Whose standards?
Mary further muses over “by whose standards would we judge if life is not worthwhile any more”, as though this is only some vague theoretical argument amongst philosophers or doctors. This is not a psychological argument, either. Under assisted dying law reform, it is only the dying individual’s world-view and circumstances that determine whether he or she feels life is worth living: not anyone else. General philosophical theory doesn’t come into it.
She further argues that assisted dying “promotes a utilitarian view of humanity”. This is not a psychological argument, either. Nor is it valid. Indeed, legalised assisted dying respects the very nature of the diversity of humanity by enabling the world-views many people hold most dear: that of making rational choices consistent with their own beliefs, values and circumstances. Some patients, for example in Oregon, are deeply religious and believe that their God is compassionate and understands and respects their choice to avoid intolerable suffering. That’s not utilitarian at all.
Harm and the Hippocratic Oath
Mary invokes the Hippocratic Oath said by her medical friends to oblige doctors to “do no harm” and that the medical role is “in healing and helping the patient to be restored to health.” This is simplistic nonsense, not a psychological argument.
Firstly, doctors do harm all the time: think of surgical procedures or chemotherapy. Many medical interventions do harm, but we accept the harm because we expect there to be a commensurately greater good as a result.
Secondly, medical practice cannot always “restore the patient to health” as Mary exclusively puts it. What then? The dying patient may judge that the unrelievable suffering they will experience along the path to death is a greater harm than dying a little earlier. And, doctors also have a primary duty to relieve suffering, which Mary doesn’t mention. What is under review is whether a doctor may participate in the relief of intolerable and unrelievable suffering— by hastening death—if the patient believes this is the lesser harm.
Thirdly, the Hippocratic Oath is around 2,300 years old. It requires doctors to swear allegiance to ancient Greek gods. It forbids women from becoming doctors. It requires current doctors to train the next generation free of charge, and it forbids surgery. Contemporary doctors don’t take it, and it’s certainly not “part of training” as Mary mistakenly states.
None of these are psychology arguments.
'Sucker’s choice'
Mary then argues that requiring dying patients to endure until the end promotes—and that assisted dying prevents—“fostering gratitude”, “reconciling hurts or differences with family members or friends” and “showing them strategies or different ways to approach their pain and suffering”.
But, in jurisdictions where assisted dying is legal, for example in Oregon in the USA, these are precisely things that are encouraged under assisted dying. Doctors are required to inform applicants of available medical and palliative interventions. Family gathers on notice of an anticipated death, music and poetry is shared, and expressions of love, devotion and gratitude are exchanged.
If a dying patient has no intention of reconciling with family or reflecting on approaches to dealing with their pain and suffering under an assisted dying law, precisely the same intention applies to the current regime that requires the patient to endure until the end. To assume a difference is a false dichotomy.
Obligatory compassion
Mary also argues that assisted dying ought to remain outlawed because “nursing a sick loved one is a way to give back”. This is yet another specious non-psychology argument. It promotes the ‘right’ of the ‘nurse’ to express love and devotion through ‘caring interventions’ at the expense of the dying patient’s own world view and deeply-held wish for a hastened death. Now who’s being utilitarian?
The upshot
I ran Mary’s opinion piece past an experienced psychologist, who described it as little to do with psychology. Note that neither of us has experience of or is commenting on Mary’s expertise as a clinical psychologist: she may indeed be a very good one.
My associate wondered out loud if Mary’s arguments were based more on underlying religious views than anything else. I agreed: they seemed to me remarkably consistent with the arguments advanced by religious opponents, even though they avoided directly religious words. So I did a little research.
It turns out that Mary is a committed and active Sydney Catholic.* Evidence abounds of her devotion to the Catholic tradition, and I commend her for her conscientious reflective practice and participation in it.
However, I argue that neither the stated psychological qualification nor the unstated religious affiliation make the offered arguments valid.
-----
* By way of fairness, I place on the record that I am agnostic.
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:13pm
The Council of Europe chamber in session.
On the 25th January 2012, the Council of Europe passed declaration 1859 on advance care planning. Immediately, lobbyists opposed to assisted dying loudly proclaimed that the resolution banned euthanasia across Europe, when it did nothing of the sort. What actually happened?
Declaration 1859 on advance care planning
The Strasbourg-based Council of Europe passed declaration 1859 on 25th January 2012. The declaration was about advance care planning, which allows patients to inform others about what treatments they would or wouldn't want if they become unable to participate in treatment decision-making.
The declaration made the explicit point that it was about advance care planning and not about euthanasia or assisted suicide. It made the point that non-voluntary euthanasia is unacceptable—that is, that others should not make death-hastening decisions about a person for their 'alleged benefit'. This is an important point on which both sides of the assisted dying debate can agree.
Council of Europe resolutions are informative to members, but are not binding.
Misstatements by opponents of assisted dying
Despite this simplicity and clarity, the very next day after the vote, a host of conservative religious organisations and commentators began trumpeting that "the Council of Europe banned euthanasia across Europe." It started with the Catholic Church (through its online service Zenit) and sprinted right around the world in a matter of days—even appearing eventually in a professional journal paper two and a half years later.
What really happened: the evidence
But no matter how often and how loudly lobbyists try to claim that the Council of Europe banned euthanasia across europe, it did nothing of the sort.
Read the forensic analysis of the misinformation trail in the F files, here.
Blog by Neil FrancisPosted on Sunday 14th June 2015 at 4:06pm
Neil Francis announces the official launch of DyingForChoice.com, the world's premier source of reliable, evidence-based information about assisted dying, and responsible law reform to permit it in restricted circumstances.
Hi, and thanks for dropping by.
I'm delighted to announce the official launch of DyingForChoice.com. The mission is to help society work towards responsible assisted dying law reform, a reform wanted by the great majority of citizens in many countries. Yet assisted dying (in one form or another) is still illegal in many jurisdictions.
DyingForChoice.com will lay out the case for restricted assisted dying including world-view arguments, but also importantly provide rigorous factual evidence and analysis. This approach is a deliberate counter-measure to mistaken information — 'misinformation', more colloquially known as 'bull' — that is available so widely and repeated so often.
Misinformation can take the form of flapdoodle, filibuster, flip-flop, fudge or outright fiction. Ultimately it's fear-mongering via the promotion of bull. Legislative reform — so that all citizens are afforded the right to enact their own deeply-held world views and cherished values at the end of life, whatever those may be — deserves to be informed by quality information.
Exposing misinformation works. Already, my exposure of the 'suicide contagion' myth has resulted in selected website 'information' being withdrawn. It's up to all of us to hold a bright spotlight up to misinformation and to ask people not to spread bull.
So subscribe to our monthly newsletter to keep abreast of developments. You can also create your own login which will allow you to comment on posts, subject of course to our terms of use. Just use the Register link in the header bar.
You can also subscribe to our Twitter feed, catch up with our Facebook page, and watch any of our videos on our YouTube channel: just click the relevant button in the header bar.
So, keep in touch, stay up to date, and if you have a burning issue you would particularly like us to report on, just send a message using our Contact form.
The F filesPosted on Tuesday 2nd June 2015 at 4:33pm
The Council of Europe chamber in session.
Here’s a clear example of mistaken information (misinformation) — more commonly known as ‘bull’ — published by conservative opponents of assisted dying law reform. In this case, lobbyists and commentators misreport by fudge: by cherry-picking and repositioning a declaration of the Council of Europe, asserting that it ‘banned euthanasia' throughout Europe.
It did nothing of the sort. So what actually happened?
In 2011, the Council’s Social, Health and Family Affairs Committee conducted a study called “Protecting human rights and dignity by taking into account previously expressed wishes of patients.” Its purpose was to make recommendations about advance care directives, and enduring powers of attorney—also known in some jurisdictions as guardianship. These are preferences, documented in advance by a person, which help ensure his or her healthcare wishes are respected and honoured at times when the person can’t currently decide and speak for him or herself. The Committee’s report was handed down as Document 12804.
Wednesday January 25th 2012
On January 25th 2012, declaration 1859 regarding the Committee’s report came before the Parliamentary Assembly of the Council of Europe (PACE) for consideration and a vote.
After most delegates had left the very lengthy session, some remaining delegates moved an amendment to the declaration. While it was procedurally their right to do so, they made the attempt only when some five sixths (268 of 318) of their Council colleagues were absent.
“an unlikely alliance of the Catholic Church and evangelicals like Pat Robertson who is behind the European Centre for Law and Justice.”
As a result, a statement mentioning euthanasia was added to the original declaration and was passed by (a tiny) vote.
You can read the entire declaration here. It’s less than two pages.
Now, what the declaration has to say about ‘euthanasia’ appears exclusively in Clause 5, and Clause 5 says in its entirety:
“5. This resolution is not intended to deal with the issues of euthanasia or assisted suicide. Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited. This resolution thus limits itself to the question of advance directives, living wills and continuing powers of attorney.”
Notice that the clause contains exactly and only three short sentences.
The first sentence is explicit and unambiguous: the declaration is not about euthanasia or assisted suicide.
The second sentence makes it abundantly clear that hastened-dying decisions made by persons other than the patient themselves but alleged to be (i.e. by others) for a ‘dependent’ patient’s ‘benefit’ are unacceptable. Declaring against such non-voluntary euthanasia is a fundamental principle on which both sides of the assisted dying debate can agree. The resolution does not speak against voluntary euthanasia: that is, when a competent patient chooses assisted dying for themselves.
The third sentence reiterates clearly that the declaration deals only with advance directives ('living wills') and continuing powers of attorney (persons granted the legal power to make decisions consistent with the advance directive). Note that the declaration wording does not even speak against assisted dying options within advance directives where permissible by law (e.g. as in the Netherlands), because these are made voluntarily by a competent patient on their own behalf and not by someone else for some 'alleged benefit’.
So, the declaration is not in conflict in any way with the laws of member states which already have assisted dying laws. Nor does it preclude other member states from introducing assisted dying laws.
Indeed, the declaration is not in conflict because the adoption of declarations by each member state is voluntary. It is incorrect to represent in any way that a Council of Europe declaration is a ‘determination,’ ‘ruling,’ ‘ban,’ ‘prohibition’ or other form of obligation upon its members.
But don’t just take my word for it.
Dr Stephen Latham, Director of the Interdisciplinary Centre for Bioethics at Yale University, states unequivocally in his blog on bioethics:
“… it’s a mistake to report it [the declaration] as a condemnation of assisted suicide, or to anticipate that it will have strong effect on pending cases involving assisted suicide.”
Dr Latham rightly points directly to the explicit declaration statement that it “is not intended to deal with the issues of euthanasia or assisted suicide." He further affirms that the European Court for Human Rights (a court of the Council of Europe) has held that Article 8 of the Convention for the Protection of Human Rights and Fundamental Freedoms protects the individual’s choice to avoid a painful and undignified death.
So, despite the clarity of the declaration, how long did it take for opponents of assisted dying to publish mistaken information about it?
Thursday January 26th 2012
Within mere hours of the vote, cherry-picked bull began charging around the globe.
Bolting energetically out of the paddock was the Catholic online newspaper promoting Vatican opinion, Zenit. Proclaiming jubilantly, “Anti-euthanasia ruling hailed as major victory”, Zenit stumbled at the first hurdle of truthfulness —the declaration was not, in any sense, a ‘ruling,’ nor called for a blanket “prohibition of euthanasia” as its lead paragraph states.[1]
Off to a similarly agile start was Dr Grégor Puppinck, Director General of the conservative Christian lobby group the European Center of Law & Justice — who you will remember David Pollock described above as in an alliance with the Catholic Church and others. Published on the Catholic Family-backed Turtle Bay and Beyond blog, this article was wrongly titled “Major victory for life in Europe: euthanasia must always be prohibited.”[2]
For good measure, Dr Puppinck’s opinion piece, complete with alternate headline “Victory: Council of Europe adopts resolution against euthanasia”, was published the same day on the USA Christian/Catholic pro-life website LifeNews.com.[3]
Similarly, Christian/Catholic pro-life website LifeSiteNews.com's John Westen published a piece the same day titled "Major victory for life in Europe: ‘Euthanasia must always be prohibited'".[4]
Also on the same day, the conservative European think tank European Dignity Watch’s headline likewise cherry-picked words from the declaration: “Council of Europe bans euthanasia”.[5]
Wasting no time, the Swedish Christian “Yes To Life” group trumpeted the mistruth “Council of Europe prevents euthanasia in Europe!” (The Council of Europe would be very talented indeed if it could actually “prevent euthanasia across Europe".)[6]
Canadian Alex Schadenberg’s Euthanasia Prevention Coalition also repeated the same cherry-picked nonsense with the headline “Council of Europe states that: ‘Euthanasia must always be prohibited.’”[7]
Friday January 27th 2012
Well-known UK Catholic journalist Simon Caldwell was only a shade slower out of the blocks just one day later. His article’s headline in UK’s Daily Mail rates a comprehensive fail for saying “Euthanasia ‘must always be prohibited’, rules Council of Europe.”[8]
Saturday 28th January 2012
Another day later and the UK Telegraph republished the story, misstating “Assisted suicide should be illegal through Europe, human rights body rules.”[9] (While this article had no by-line, its copy was remarkably identical to Simon Caldwell’s pieces in the Daily Mail [above] and UK Catholic Herald [below]. Caldwell is a known writer for the Telegraph.)
Monday 30th January 2012
Simon Caldwell followed up with the same article in the UK Catholic Herald, again with a false headline “Euthanasia should be banned across Europe, rules Council.”[10]
Also on 30th January, Catholic-founded Australian Family Association's Paul Russel uncritically republished Alex Schadenberg’s opinion piece on their anti-voluntary euthanasia campaign site “HOPE”.[11]
Tuesday 31st January 2012
Not to be outdone, the next day the Patients Rights Council (formerly the International Task Force on Euthanasia and Assisted Suicide), an anti-euthanasia lobby group consisting essentially of two people (Rita Marker and Wesley Smith), uncritically summarised Simon Caldwell’s Daily Mail opinion piece.[12]
Wednesday February 1st 2012
On February 1st the polemic was republished in CathNews in Australia, with false headline “Council of Europe says ban euthanasia.”[13]
The Catholic Archdiocese of Sydney republished on its youth engagement website xt3, with the headline “Euthanasia should be banned across Europe, rules Council.”[14]
Friday February 3rd 2012
By February 3rd, the Church of England Newspaper had jumped on the bandwagon, misstating “Council of Europe assemby [sic] calls for ban on euthanasia.”[15]
So did the Scottish Catholic Observer with an extra dose of hyperbole: “European human rights body rules that euthanasia and assisted suicide should be banned in every country on the continent.”[16]
No wonder Yale University’s Dr Latham mused dryly in his blog:
“… a number of different publicationsare mistakenly alleging that PACE has called for a permanent ban on assisted suicide.”
September 19th 2012
Later in the year I was kindly invited to speak at a Brisbane public forum on the legalisation of voluntary euthanasia hosted by the Queensland Council for Civil Liberties. Mr Yuri Koszarycz, then recently retired lecturer in bioethics, ethics and church history from Australian Catholic University, spoke for the opposing position. Given the audience were paying to listen to our respective pearls of wisdom, it was paramount that our material be properly researched and backed by good evidence.
Yet Mr Koszarycz dropped the “R” bomb (amongst others) in his presentation: yes, he asserted that the Council of Europe had ‘ruled’ against euthanasia, when it clearly had not.
July 17th 2014
Dr Grégor Puppinck (remember, he’s Director General of the European Center of Law & Justice) makes another appearance, this time as the lead author of a paper published in the International Journal of Human Rights[17]. In it, he rails against his perception that when reviewing cases of assisted suicide, the European Court of Human Rights ‘ignores’ Council of Europe declaration 1859. To support his argument, he quotes the single sentence “Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited” (p 746).
The paper’s discussion quite omits the two crucial, framing sentences, so a reader unfamiliar with the declaration’s original text would not know that it said it is “not intended to deal with the issues of euthanasia or assisted suicide” and that it is about “living wills and continuing powers of attorney”. No wonder the European Court of Human Rights doesn’t believe that declaration 1859 is crucial when considering cases of assisted suicide: declaration 1859 is about advance care planning!
Indeed, a reader of the journal article could be forgiven for wrongly deducing, on the basis of the only sentence quoted by authors Puppinck and de la Hougue, that the Council had ‘banned euthanasia’. It most certainly had not.
Conclusion
So let’s recap what happened. The primary facts are:
The Council of Europe passed a declaration (#1859) about advance care planning—not about euthanasia or assisted suicide (it explicitly said it wasn't).
The declaration spoke only against non-voluntaryeuthanasia (NVE)—not against voluntary euthanasia (VE) about which it contained no statement of any kind.
Council declarations are in no way 'rulings', 'bans' or 'prohibitions' on its members because member adoption is entirely voluntary.
Yet despite the clarity of the declaration, quite a number of anti-euthanasia lobby groups and commentators, commencing the very next day and starting with the Catholic Church (through Zenit) and the European Centre for Law and Justice, published editorials mistakenly stating that the Council of Europe had ‘banned euthanasia': in other words, spreading bull.
A question that could be asked is this: how did it happen that so many anti-euthanasia individuals and groups published misstatements so closely together in both interpretation and in time?
[17] Puppinck, G & de La Hougue, C 2014, 'The right to assisted suicide in the case law of the European Court of Human Rights', International Journal of Human Rights, vol. 18, no. 7-8, pp. 735-755.
 Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
 Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.